Abstract
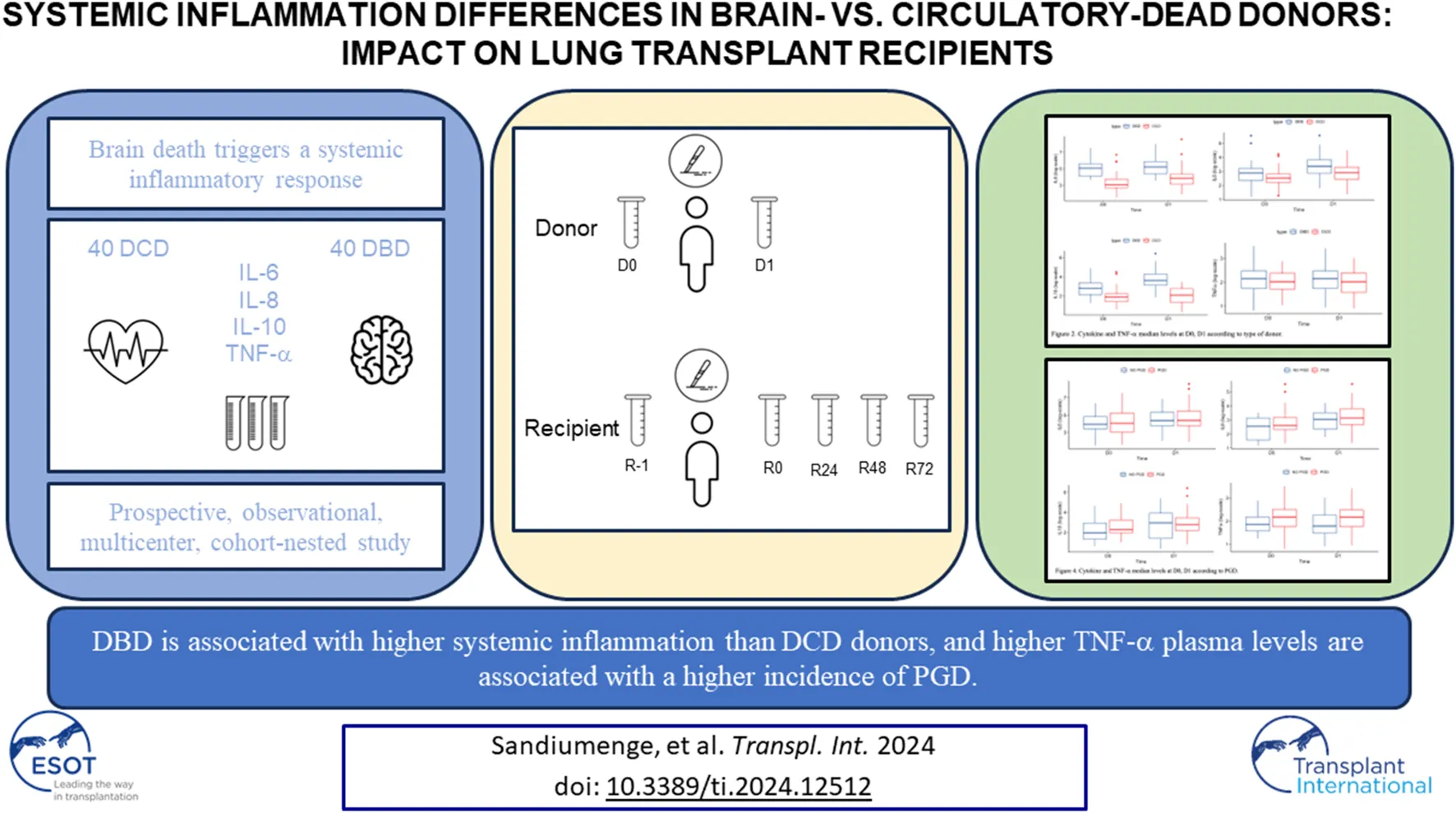
Brain death triggers a systemic inflammatory response. Whether systemic inflammation is different in lung donors after brain- (DBD) or circulatory-death (DCD) is unknown, but this may potentially increase the incidence of primary graft dysfunction (PGD) after lung transplantation. We compared the plasma levels of interleukin (IL)-6, IL-8, IL-10 and TNF-α in BDB and DCD and their respective recipients, as well as their relationship with PGD and mortality after LT. A prospective, observational, multicenter, comparative, cohort-nested study that included 40 DBD and 40 DCD lung donors matched and their respective recipients. Relevant clinical information and blood samples were collected before/during lung retrieval in donors and before/during/after (24, 48 and 72 h) LT in recipients. Incidence of PGD and short-term mortality after LT was recorded. Plasma levels of all determined cytokines were numerically higher in DBD than in DCD donors and reached statistical significance for IL-6, IL-10 and IL-8. In recipients with PGD the donor’s plasma levels of TNF-α were higher. The post-operative mortality rate was very low and similar in both groups. DBD is associated with higher systemic inflammation than DCD donors, and higher TNF-α plasma levels in donors are associated with a higher incidence of PGD.
Introduction
Donation after brain death (DBD) is the main source of organ donation for transplantation worldwide. Brain death (BD) usually induces a systemic inflammatory response. This “cytokine storm” may damage different body organs in donors, which may in turn have a deleterious impact on their function and survival in recipients after transplantation [–] since this can further aggravate the insults that occur during warm and cold ischemia and the subsequent reperfusion of the transplanted organ, by amplifying an inflammatory response in the recipient []. Lungs are especially sensitive to the BD-induced cytokine storm, which enhances the likelihood of ischemia-reperfusion-induced primary graft dysfunction (PDG) []. PDG is one of the main complication during the early post-operative period of lung transplantation and is the first cause of mortality during the first month and second one during the first year after transplantation [] significant morbidity, as well as longer hospital length of stay and duration of mechanical ventilation. Experimental evidence has strongly suggested that DBD increases the incidence and severity of PGD(3,7).
Given the shortage of DBD donors, in recent years, donation after circulatory death (DCD) has been increasingly used as a source of organs for transplantation. The cytokine storm that follows BD and the potential deleterious impact on the lungs could theoretically be prevented or minimized during a DCD process []. Based on previous studies, we hypothesized that the plasma level of several inflammatory cytokines would be higher in DBD vs. DCD. To test this hypothesis, we conducted a prospective study that sought to compare: (1) the plasma levels of the pro-inflammatory (IL-6, IL-8, TNF-α) and anti-inflammatory cytokines (IL-10) in BDD vs. DCD; (2) the plasma levels of pro-inflammatory (IL-6, IL-8, TNF-α) and anti-inflammatory cytokines (IL-10) in recipients with PGD; and (3) the incidence of PGD and short-term mortality in LT recipients from DBD or DCD.
Material an Methods
Study Design and Ethics
This was a prospective, observational cohort-nested study conducted in four transplant centers in Spain that included adult patients undergoing uni- or bilateral LT between July 2018 and July 2019 and their respective BD or CD donors. The type of death was certified in accordance with Spanish legislation25.
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the Human Research Committees of all participating hospitals (PR [AG]202/2017). All recipients provided written informed consent before being included in the study. Informed consent to participate in the study from donors was included in the donation consent. No deviation from the standard management of lung recipients took place except for serial blood sampling.
Patients
LT recipients from DBD and DCD were matched individually for sex, age (±5 years), and indication for LT (Figure 1). We excluded from this analysis patients undergoing lung re-transplantation, cardiopulmonary transplantation or those who had previously undergone or were to receive more than one simultaneous solid organ transplantation, as well as those for whom the graft ischemic time was >420 min. Following previous reports by Koukoulis et al.27 and considering a confidence interval of 95%, statistical power of 80% and patient loss of 15%, a sample size of 36 LT recipients for each group (DCD and DBD) was estimated to detect a difference of at least one SD (15 pg/mL) in IL-6 plasma levels.
FIGURE 1
Study Variables
The following donor and recipient variables were prospectively collected: demographic (sex, age) and anthropometric (body mass index) measurements; clinical data (cause of death, corticosteroid pretreatment of donors and indication for transplantation of recipients); and surgical data (transfusion of blood products, vasoactive support or application of veno-venous [VV-] or veno-arterial [VA-] extracorporeal membrane oxygenation [ECMO], ischemic times for the first and second lungs and use of cardiopulmonary bypass). In all recipients, we registered the development of PGD (any grade and grade III) within 72 h post-transplantation according to the International Society for Heart and Lung Transplantation (ISHLT) Working Group criteria []. Mortality during the first 3 months after the transplant was also recorded.
Measurements
Blood samples (10 mL) were obtained from donors before skin incision (D0) and before organ perfusion (D1). In recipients, blood samples were obtained in the operating room before implantation surgery (R-1), just after graft reperfusion (R0) and 24 (R24), 48 (R48) and 72 (R72) hours after LT. All blood samples were collected in EDTA tubes and centrifuged at 1,000 g for 10 min at room temperature (22ºC–23°C). Plasma was separated, divided into 2 aliquots of 2 mL each, and immediately stored at −80°C until analysis. At the end of the inclusion period, samples were shipped together in dry ice containers to the central laboratory located at the coordinating site (Hospital Universitari Vall d’Hebron, Barcelona) for cytokine analysis by immunofluorescence assays based on microfluidics using ELLA Simple Plex (Protein Simple, Biotechne, CA, United States) to simultaneously detect IL-6, IL-10, IL-8 and TNF-α. Triplicates of each cytokine result were obtained (the maximum allowed variation among triplicates was 5%).
Data Analysis
Data were collected and stored in an ad hoc database on the website of the Organización Nacional de Trasplantes (ONT, Spanish Transplant Organization) and made accessible only to the principal investigator of each participating site. A member of the ONT was commissioned to monitor the study.
The Shapiro-Wilk test was performed as a test of normality for IL level distribution. Categorical variables are expressed as n and percentages. Quantitative data is presented as mean ± SD if normally distributed or as median (Q1, Q3) if not. Chi-square test, or Fisher’s exact test were used to compare categorical variables. Change over time was analyzed with non-parametric 2-way mixed repeated-measures ANOVA. The basic model included a group factor (DBD or DCD), a time factor, and an interaction between group and time. The main effects of group and time were explored for nonsignificant interactions. Bonferroni correction was applied to adjust for multiple comparisons in posthoc tests to determine specific pairwise differences between groups. All statistical analyses were performed using R version 4.3.1 (R Core Team, 2023). A p-value < 0.05 was considered statistically significant.
Results
Patient Characteristics
Figure 1 presents the consort diagram of the study. A total of 156 LT recipients were initially included, but 24 were later excluded because of incomplete data. Of the remaining 132 patients, 106 were DBD recipients and 40 were DCD recipients. Forty of the 106 DBD recipients were matched individually to the 40 DCD ones by sex, age (±5 years) and indication for lung transplantation.
Table 1 contrasts the main characteristics of both donors and recipients. More DBD received corticosteroids and vasoactive support before lung retrieval than DCD (p = 0.02 and p = 0.043, respectively), while more DCD than DBD received transfusions of blood products (p = 0.001). No other significant differences were observed between groups in donor or recipient characteristics.
TABLE 1
| DBD | DCD | p -value | ||
|---|---|---|---|---|
| (n = 40) | (n = 40) | |||
| Donor | Sex, male, n (%) | 22 (55) | 18 (45) | 0.799 |
| Age, years, mean ± SD | 54 ± 16 | 56 ± 14 | 0.435 | |
| BMI, kg/m2, mean ± SD | 26 ± 5 | 26 ± 5 | 0.754 | |
| Corticosteroids treatment, n (%) | 35 (87.5) | 22 (55) | 0.002 | |
| Transfusion with blood products, n (%) | 2 (5) | 8 (20) | 0.043 | |
| Vasoactive drugs treatment, n (%) | 34 (85) | 12 (30) | 0.001 | |
| VV- or VA-ECMO, n (%) | 0 (0) | 4 (10) | 0.116 | |
| Cause of death, n (%) | 0.014 | |||
| Stroke | 31 (77.5) | 19 (47.5) | ||
| Anoxia | 3 (7.5) | 13 (32.5) | ||
| Traffic head injury | 2 (5) | 1 (2.5) | ||
| Traffic non head injury | 4 (10) | 4 (10) | ||
| Other | 0 (0) | 3 (7.5) | ||
| Recipient | Sex, male, n (%) | 23 (57.5) | 24 (60) | 0.820 |
| Age, years, mean ± SD | 56 ± 10 | 54 ± 10 | 0.500 | |
| BMI kg/m2± SD | 25 ± 4 | 24 ± 4 | 0.189 | |
| Ischemic time 1st graft, min, mean ± SD | 238 ± 61 | 256 ± 48 | 0.213 | |
| Ischemic time 2nd graft, min, mean ± SD | 341 ± 82 | 353 ± 56 | 0.213 | |
| Cardiopulmonary bypass, n (%) | 20 (20) | 7 (17.5) | 0.775 | |
| Transfusion with blood products, n (%) | 27 (67.5) | 19 (47.5) | 0.070 | |
| Vasoactive drugs intake, n (%) | 33 (82.5) | 35 (87.5) | 0.630 | |
| VV- or VA-ECMO after transplantation, n (%) | 2 (5) | 4 (10) | 0.675 | |
| Indication for lung transplantation (%) | - | |||
| Bronchiectasis | 3 (7.5) | 3 (7.5) | ||
| Diffuse interstitial lung disease | 17 (42.5) | 18 (45) | ||
| Occupational lung disease | 1 (2.5) | 1 (2.5) | ||
| COPD/Emphysema | 12 (30) | 11 (27.5) | ||
| Cystic fibrosis | 3 (7.5) | 3 (7.5) | ||
| Pulmonary hypertension | 3 (7.5) | 3 (7.5) | ||
| Other | 1 (2.5) | 1 (2.5) |
Donor and recipient characteristics.
BMI: body mass index; COPD, chronic obstructive pulmonary disease; ECMO: extracorporeal membrane oxygenation; VA: veno-arterial; VV: veno-venous.
Systemic Inflammation
At D0 and D1 the levels of IL-6, IL-10 and IL-8 were higher in the DBD group than in DCD, and a significant main effect of time with a higher concentrations at D1 compared to D0 with statistical significant increase the IL-10 levels at D1 in DBD group. There was no statistical differences of type or time on TNFα (Table 2; Figure 2).
TABLE 2
| D0 | D1 | p-values | |||||
|---|---|---|---|---|---|---|---|
| DBD | DCD | DBD | DCD | p:time | p:type | p:interaction | |
| IL10 | 16.4 (8.6, 29.0) | 6.8 (4.2, 9.4) | 37.9 (22.8, 73.7) | 8.1 (4.0, 15.9) | <0.001 | <0.001 | 0.004 |
| IL 6 | 164.3 (61.9, 278.9) | 21.1 (15.1, 43.2) | 189.4 (81.5, 363.3) | 46.5 (23.0, 76.3) | 0.040 | 0.003 | 0.381 |
| IL 8 | 18.1 (11.3, 25.3) | 12.5 (9.1, 16.5) | 28.6 (17.5, 45.7) | 18.5 (11.3, 27.4) | <0.001 | 0.010 | 0.210 |
| TNF α | 8.6 (5.7, 11.9) | 7.5 (5.6, 10.7) | 8.6 (5.7, 11.8) | 7.5 (4.9, 10.8) | 0.883 | 0.479 | 0.467 |
Levels (pg/mL) of cytokines according to the type of donor at D0 and D1. Data expressed as median (Q1, Q3). p-values corresponding to non-parametric two-way mixed ANOVA.
FIGURE 2
In recipients, there was no statistical significance of type of donor on IL-6, IL-10, IL-8 and TNF. Before LT (R-1), the plasma level of these cytokines was similar in both groups (DBD and DCD) and immediately after LT (R0), the plasma levels of IL-6, IL-8 and IL-10, increased in both groups of recipients and decreased thereafter during the next 72 h without differeces. There was a statistically significant effect of time on TNFα only for the DBD group (Table 3; Figure 3).
TABLE 3
| R-1 | R0 | R24 | R48 | R72 | p-values | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DBD | DCD | DBD | DCD | DBD | DCD | DBD | DCD | DBD | DCD | p:time | p:type | p:interaction | |
| IL10 | 2.9 (2.3, 4.3) | 2.4 (1.9, 3.2) | 151.6 (63.7, 624.0) | 233.3 (69.2, 397.4) | 17.4 (11.4, 24.1) | 14.9 (9.8, 25.4) | 7.9 (5.3, 10.5) | 7.8 (6.3, 11.5) | 7.9 (5.4, 10.8) | 6.6 (4.6, 10.1) | <0.001 | 0.947 | 0.614 |
| IL 6 | 8.1 (3.1, 23.7) | 4.0 (2.1, 8.1) | 329.2 (244.3, 848.8) | 352.5 (107.4, 565.9) | 56.7 (35.7, 93.4) | 58.0 (41.6, 89.1) | 25.3 (17.1, 39.9) | 29.2 (18.9, 59.5) | 19.9 (10.1, 30.7) | 15.7 (8.9, 21.6) | <0.001 | 0.293 | 0.146 |
| IL 8 | 14.8 (8.8, 29.0) | 12.3 (8.2, 17.6) | 56.2 (35.2, 119.0) | 46.7 (19.1, 114.7) | 12.7 (8.2, 21.8) | 13.3 (9.0, 33.5) | 10.6 (7.9, 16.2) | 11.0 (8.0, 19.8) | 12.3 (8.5, 16.7) | 11.5 (8.0, 14.4) | <0.001 | 0.706 | 0.361 |
| TNF α | 5.9 (5.2, 7.3) | 5.0 (4.1, 6.5) | 7.1 (5.1, 10.1) | 5.2 (4.1, 6.8) | 4.8 (3.5, 6.7) | 5.4 (3.7, 6.6) | 4.9 (4.1, 7.9) | 5.3 (4.0, 7.2) | 6.2 (4.7, 9.8) | 4.9 (3.7, 6.5) | 0.062 | 0.069 | 0.005 |
Levels (pg/mL) of cytokines according to the type of donor at R-1 to R72. Data expressed as median (Q1, Q3). p-values corresponding to non-parametric two-way mixed ANOVA.
FIGURE 3
Primary Graft Dysfunction (PGD)
The incidence of PGD of any grade was similar in DCD and DBD recipients (Table 4). Therefore, to further investigate the evolution of systemic inflammation in PGD we merged both groups for analysis. We found that the donor plasma levels of all cytokines were comparable between patients who developed any grade of PGD or not, except for TNF-α, which was higher at D0 and D1 in those recipients with PGD (Table 5; Figure 4). Specific analysis of PGD grade 3 did not show differences between groups (Table 6).
TABLE 4
| DBD | DCD | p -value | |
|---|---|---|---|
| (n = 40) | (n = 40) | ||
| Primary graft dysfunction, n (%) | |||
| Of any grade | 27 (67.5) | 26 (65) | 0.100 |
| Grade III | 14 (35) | 11 (27.5) | 0.469 |
| Post-operative mortality | 0 (0) | 2 (5) | 0.494 |
| Three-month mortality | 0 (0) | 2 (5) | 0.494 |
Outcomes after lung transplantation from DBD and DCD.
TABLE 5
| D0 | D1 | p-values | |||||
|---|---|---|---|---|---|---|---|
| No PGD | PGD | No PGD | PGD | p:time | p:PGD | p:interaction | |
| IL10 | 7.0 (3.8, 18.9) | 9.7 (7.2, 25.4) | 19.2 (4.0, 50.0) | 15.9 (8.8, 32.1) | 0.018 | 0.903 | 0.291 |
| IL 6 | 51.8 (30.4, 124.7) | 58.2 (21.3, 188.6) | 78.5 (43.5, 209.0) | 81.8 (44.8, 237.5) | 0.003 | 0.773 | 0.314 |
| IL 8 | 12.9 (4.9, 23.1) | 14.1 (10.3, 24.2) | 21.1 (10.6, 33.5) | 23.2 (14.6, 45.1) | <0.001 | 0.226 | 0.555 |
| TNF α | 6.4 (4.8, 8.8) | 8.8 (5.8, 12.3) | 6.0 (4.4, 9.5) | 8.7 (5.8, 12.0) | 0.769 | 0.022 | 0.648 |
Levels (pg/mL) of cytokines according to PGD at D0 and D1. Data expressed as median (Q1, Q3). p-values corresponding to non-parametric two-way mixed ANOVA.
FIGURE 4
TABLE 6
| D0 | D1 | p-values | |||||
|---|---|---|---|---|---|---|---|
| No PGD/PGD12 | PGD3 | No PGD/PGD12 | PGD3 | p:time | p:PGD3 | p:interaction | |
| IL10 | 8.8 (5.8, 23.2) | 9.2 (6.8, 23.8) | 20.6 (7.9, 40.7) | 14.8 (6.4, 28.2) | 0.001 | 0.419 | 0.040 |
| IL 6 | 48.4 (20.9, 112.0) | 164.3 (38.3, 302.2) | 68.2 (35.7, 194.9) | 125.8 (60.5, 443.6) | 0.165 | 0.091 | 0.595 |
| IL 8 | 13.0 (9.0, 22.7) | 16.4 (10.2, 26.0) | 19.9 (11.6, 34.3) | 27.1 (17.1, 50.2) | <0.001 | 0.099 | 0.090 |
| TNF α | 7.0 (5.4, 10.5) | 9.3 (6.0, 11.6) | 7.4 (4.9, 11.8) | 9.6 (6.4, 11.3) | 0.182 | 0.618 | 0.615 |
Levels (pg/mL) of cytokines according to PGD0-2 vs. PGD3 at D0 and D1. Data expressed as median (Q1, Q3). p-values corresponding to non-parametric two-way mixed ANOVA.
On the other hand, recipients experiencing PGD demonstrated elevated levels of IL-6 at R0 and a trend towards R48 and IL-8 at R0, R48, without differences between groups (Table 7; Figure 5). Furthermore, in the PGD grade 3 group, recipient plasma levels of IL-6 and IL-8 were significantly elevated at R0, R24 and R48 (Table 8).
TABLE 7
| R-1 | R0 | R24 | R48 | R72 | p-values | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No PGD | PGD | No PGD | PGD | No PGD | PGD | No PGD | PGD | No PGD | PGD | p:time | p:PGD | p:interaction | |
| IL10 | 2.6 (1.9, 3.1) | 2.9 (2.2, 4.4) | 146.5 (44.1, 402.0) | 184.9 (95.7, 409.6) | 13.3 (10.0, 20.5) | 19.0 (12.0, 28.1) | 7.0 (5.3, 9.6) | 8.4 (6.2, 11.7) | 7.6 (4.9, 12.1) | 7.3 (5.2, 9.6) | <0.001 | 0.654 | 0.212 |
| IL 6 | 3.9 (2.4, 15.3) | 4.7 (2.9, 12.6) | 205.2 (79.1, 407.5) | 462.9 (269.4, 792.3) | 51.0 (33.6, 71.9) | 63.6 (43.5, 99.2) | 20.7 (14.8, 38.1) | 28.5 (20.7, 52.7) | 17.1 (7.2, 28.2) | 17.7 (10.8, 27.0) | <0.001 | 0.009 | 0.114 |
| IL 8 | 13.1 (9.0, 19.6) | 12.8 (8.2, 24.1) | 30.2 (16.2, 52.1) | 67.1 (35.9, 120.4) | 11.4 (8.5, 14.5) | 13.5 (9.9, 27.5) | 9.4 (7.0, 12.7) | 11.6 (8.7, 21.2) | 11.0 (7.9, 14.1) | 12.4 (9.0, 15.8) | <0.001 | 0.003 | 0.068 |
| TNF α | 5.0 (4.2, 5.8) | 5.7 (4.6, 7.0) | 5.8 (4.0, 10.3) | 5.6 (4.7, 8.8) | 4.4 (3.1, 6.8) | 5.3 (3.9, 6.3) | 4.9 (4.0, 8.3) | 5.2 (4.2, 6.8) | 5.4 (4.5, 8.3) | 5.3 (4.2, 7.1) | 0.132 | 0.927 | 0.617 |
Levels (pg/mL) of cytokines according to PGD at R-1 to R72. Data expressed as median (Q1, Q3). p-values corresponding to non-parametric two-way mixed ANOVA.
FIGURE 5
TABLE 8
| R-1 | R0 | R24 | R48 | R72 | p-values | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No PGD/PGD12 | PGD3 | No PGD/PGD12 | PGD3 | No PGD/PGD12 | PGD3 | No PGD/PGD12 | PGD3 | No PGD/PGD12 | PGD3 | p:time | p:PGD3 | p:interaction | |
| IL10 | 2.6 (2.0, 3.2) | 2.7 (1.9, 4.3) | 200.8 (44.9, 477.2) | 160.6 (96.6, 290.4) | 15.4 (10.0, 22.5) | 22.0 (14.4, 33.2) | 7.7 (5.7, 9.7) | 9.2 (6.8, 18.8) | 7.1 (4.9, 10.3) | 7.7 (6.3, 10.4) | <0.001 | 0.576 | 0.321 |
| IL 6 | 4.1 (2.7, 12.8) | 5.2 (3.0, 13.3) | 262.3 (101.1, 581.8) | 441.0 (324.0, 1153.8) | 53.3 (35.6, 78.0) | 79.3 (44.7, 104.3) | 25.3 (16.8, 55.2) | 27.7 (23.6, 44.5) | 17.3 (9.9, 27.8) | 18.5 (9.6, 25.7) | <0.001 | 0.063 | 0.097 |
| IL 8 | 12.2 (8.6, 19.2) | 17.2 (8.3, 30.0) | 42.3 (20.1, 88.9) | 74.1 (48.1, 128.5) | 11.8 (8.4, 16.1) | 20.4 (11.8, 37.8) | 10.1 (7.6, 14.4) | 15.0 (10.6, 27.3) | 11.2 (8.4, 13.8) | 13.7 (8.5, 19.6) | <0.001 | 0.010 | 0.315 |
| TNF α | 5.4 (4.5, 6.7) | 5.9 (5.1, 7.4) | 5.5 (4.3, 9.2) | 5.9 (4.7, 8.9) | 4.6 (3.2, 6.5) | 5.6 (4.3, 7.3) | 5.0 (4.0, 7.1) | 5.4 (4.2, 7.5) | 5.2 (4.3, 7.6) | 5.8 (4.1, 7.0) | 0.270 | 0.374 | 0.834 |
Levels (pg/mL) of cytokines according to PGD0-2 vs. PGD3 at R-1 to R72. Data expressed as median (Q1, Q3). p-values corresponding to non-parametric two-way mixed ANOVA.
Mortality
Post-operative mortality rate was very low and similar in both groups without any additional deaths within 3 months after surgery (Table 4).
Discussion
The main results of this prospective, controlled, multicenter, cohort-nested study are that: (1) DCD presents lower systemic inflammation than DBD in donors; (2) after LT, the time course of systemic, the incidence of PGD and mortality after LT is similar in BDB and DCD recipients; and (3)recipients from donors with elevated levels of tumor necrosis factor-alpha (TNF-α) have a higher incidence of PGD and PGD grade 3 with elevated levels of IL-6 and IL-8. These observations support the DCD as a viable LT option.
To our knowledge, this is the first prospective multicenter study comparing systemic inflammation, PGD and mortality in LT recipients according to DCD vs. DBD donors. Yet, previous experimental studies have shown the development of systemic inflammation following BD [, , ] Also, it is known that increased systemic inflammation may worsen ischemia-reperfusion-induced lung injury [, ], and has been associated with a higher incidence of PGD [, ]. Our results confirm that cytokine levels are increased after BD.
The first goal of this study was to investigate if the systemic inflammatory response elicited in DBD or DCD was different. We found that the plasma levels of IL-6, IL-8, IL-10, all well-established inflammatory markers [] were higher in donors (D1) in DBD than in DCD. Of note, this occurred despite DBD had been treated with systemic corticosteroids more often. The role of treatment with corticosteroids in the management of DCD is a matter of debate [] although it is widely used in practice. So far, only two experimental studies have indicated that it significantly reduces the plasma levels of several pro-inflammatory cytokines, warm ischemic injury [] or myocardial edema []. However, these studies were conducted during ex vivo lung perfusion. Our results in real clinical practice suggest a small role for corticosteroid treatment in preventing systemic inflammation in lung DCD.
The second goal of our study was to compare the relationship of systemic inflammation with the incidence of PGD and short-term mortality in LT recipients from DBD and DCD donors. The relationship of PGD and systemic inflammation is a controversial issue since some previous studies have reported such a relationship [, –] whereas others did not []. We observed that recipients who presented PGD were transplanted from donors with elevated levels of TNF-α.
Finally, we found that lung reperfusion was followed by a rapid and similar increase in IL-6, IL-8 and IL-10 (not TNF-α) plasma levels in DBD and DCD recipients, followed by a reduction to normal levels in the next few hours, with a similar pattern in the two groups. These similarities likely explain why the incidence of PGD and mortality rate was not different in our study between DBD or DCD.
Our results may have clinical implications because they clearly show that DCD is not associated with increased systemic inflammation (as compared to DBD) and that the incidence of PGD and post-operative mortality seemed to be similar in LT recipients from DBD or DCD donors. This provides further support for the feasibility and safety of LT from DCD donors which, in turn, can stimulate DCD donation and contribute to alleviate the shortage of DBD donors and waiting lists.
The prospective, cohort-nested design of our study and the provision of the inflammatory status of donors before lung retrieval are strengths of our study. Among potential limitations we acknowledge that, although we estimated the needed sample size based on one of the most prominent cytokines investigated here (IL6), our results need to be replicated in other larger cohorts.
Brain death in humans is associated with higher levels of IL-6, IL-8 and IL-10, but this does not alter the biologic or clinical response of LT recipients. Yet, recipients transplanted from donors with higher TNF-α plasma levels (irrespective of DBD or DCD) have an increased incidence of PGD. These observations support the use of DCD in clinical practice.
Statements
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Human Research Committees of all participating hospitals (PR[AG]202/2017). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
IB, AS, EC, and TP participated in the design, interpretation of the studies and analysis of the data; all authors conducted the experiments and review of the manuscript, IB and AS wrote the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare(s) financial support was received for the research, authorship, publication of this article. The author(s) declare(s) that this work was performed with the financial support of Fundación Invest. Médica Mutua Madrileña Ref: AP167192017.
Acknowledgments
Authors thank Leví Nuñez del Barrio, Anna Elena Gil Martinez, Ivette Castellnou Asens, Isshak Mrabet Deraoui, Elena Bechtold Javier, Beatriz Carrillo Cubero, Freddy Chilán Santana, Sonia Ramon-Cortes, Hermes Salvatore Dallo, Alba Gómez del Pulgar Martínez, Lucas Lozano Ramos, María Figueras Ravell, Christian Surós Álvarez, Sonia López Montero, from the Teaching Unit of the Vall d’Hebron Universitary Hospital–Autonomous University of Barcelona (Spain) for their contribution in the collection and processing of the blood samples.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1.
SmithM. Physiologic Changes during Brain Stem Death--Lessons for Management of the Organ Donor. J Heart Lung Transpl (2004) 23(9 Suppl. l):S217–22. 10.1016/j.healun.2004.06.017
2.
AvlonitisVSWigfieldCHGolledgeHDRKirbyJADarkJH. Early Hemodynamic Injury during Donor Brain Death Determines the Severity of Primary Graft Dysfunction after Lung Transplantation. Am J Transpl (2007) 7(1):83–90. 10.1111/j.1600-6143.2006.01593.x
3.
PratschkeJWllhelmMJKusakaMBaskerMCooperDKCHancockWWet alBrain Death and its Influence on Donor Organ Quality and Outcome after Transplantation. Transplantation (1999) 67(3):343–8. 10.1097/00007890-199902150-00001
4.
BaciuCSageAZamelRShinJBaiXHHoughOet alTranscriptomic Investigation Reveals Donor-Specific Gene Signatures in Human Lung Transplants. Eur Respir J (2021) 57(4):2000327. 10.1183/13993003.00327-2020
5.
KangCHAnrakuMCypelMSatoMYeungJGharibSAet alTranscriptional Signatures in Donor Lungs from Donation after Cardiac Death vs after Brain Death: A Functional Pathway Analysis. J Heart Lung Transplant (2011) 30(3):289–98. 10.1016/j.healun.2010.09.004
6.
ChambersDCCherikhWSHarhayMOHayesDHsichEKhushKKet alThe International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-Sixth Adult Lung and Heart–Lung Transplantation Report—2019; Focus Theme: Donor and Recipient Size Match. J Heart Lung Transplant (2019) 38(10):1042–55. 10.1016/j.healun.2019.08.001
7.
WongALiuM. Inflammatory Responses in Lungs from Donation after Brain Death: Mechanisms and Potential Therapeutic Targets. J Heart Lung Transplant (2021) 40(9):890–6. 10.1016/j.healun.2021.03.010
8.
SnellGIYusenRDWeillDStrueberMGarrityEReedAet alReport of the ISHLT Working Group on Primary Lung Graft Dysfunction, Part I: Definition and Grading—A 2016 Consensus Group Statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant (2017) 36(10):1097–103. 10.1016/j.healun.2017.07.021
9.
WongALiuM. Inflammatory Responses in Lungs from Donation after Brain Death: Mechanisms and Potential Therapeutic Targets. J Heart Lung Transpl (2021) 40(9):890–6. 10.1016/j.healun.2021.03.010
10.
de PerrotMLiuMWaddellTKKeshavjeeS. Ischemia-Reperfusion-Induced Lung Injury. Am J Respir Crit Care Med (2003) 167(4):490–511. 10.1164/rccm.200207-670SO
11.
LeeJCChristieJD. Primary Graft Dysfunction. Proc Am Thorac Soc (2009) 6(1):39–46. 10.1513/pats.200808-082GO
12.
SuzukiYCantuEChristieJD. Primary Graft Dysfunction. Semin Respir Crit Care Med (2013) 34(3):305–19. 10.1055/s-0033-1348474
13.
PhamSMYoshidaYAebaRHattlerBGIwakiYZeeviAet alInterleukin-6, a Marker of Preservation Injury in Clinical Lung Transplantation. J Heart Lung Transpl (1992) 11(6):1017–24.
14.
D'AragonFBelley-CoteEAgarwalAFrenetteAJLamontagneFGuyattGet alEffect of Corticosteroid Administration on Neurologically Deceased Organ Donors and Transplant Recipients: AEffect of Corticosteroid Administration on Neurologically Deceased Organ Donors and Transplant Recipients: A Systematic Review and Meta-Analysis. BMJ Open. 2017;7(6):e014436. 10.1136/bmjopen-2016-014436
15.
MartensABoadaMVanaudenaerdeBMVerledenSEVosRVerledenGMet alSteroids Can Reduce Warm Ischemic Reperfusion Injury in a Porcine Donation after Circulatory Death Model with Ex Vivo Lung Perfusion Evaluation. Transpl Int (2016) 29(11):1237–46. 10.1111/tri.12823
16.
SandhaJKWhiteCWMüllerAAveryEThliverisJDixonIMCet alSteroids Limit Myocardial Edema during Ex Vivo Perfusion of Hearts Donated after Circulatory Death. Ann Thorac Surg (2018) 105(6):1763–70. 10.1016/j.athoracsur.2018.01.004
17.
Fishera. JDonnellySCHiraniNHaslettCStrieterRMDarkJHet alElevated Levels of Interleukin-8 in Donor Lungs Is Associated with Early Graft Failure after Lung Transplantation. Am J Respir Crit Care Med (2001) 163(1):259–65. 10.1164/ajrccm.163.1.2005093
18.
AlmenarMCerónJGómezMDPeñalverJCJiménezMJPadillaJ. Interleukin 8 Concentrations in Donor Bronchoalveolar Lavage: Impact on Primary Graft Failure in Double Lung Transplant. Arch Bronconeumol (2009) 45(1):12–5. 10.1016/j.arbres.2008.02.004
19.
MathurABazMStaplesEDBonnellMSpeckmanJMHessPJet alCytokine Profile after Lung Transplantation: Correlation with Allograft Injury. Ann Thorac Surg (2006) 81(5):1844–9. 10.1016/j.athoracsur.2005.11.053
20.
MorenoIVicenteRRamosFVicenteJLBarberáM. Determination of Interleukin-6 in Lung Transplantation: Association with Primary Graft Dysfunction. Transpl Proc (2007) 39(7):2425–6. 10.1016/j.transproceed.2007.07.056
21.
RechTHCustódioGKrothLVHenrichSFFilhoÉMRCrispimDet alBrain Death-Induced Cytokine Release Is Not Associated with Primary Graft Dysfunction: A Cohort Study. Rev Bras Ter Intensiva (2019) 31(1):86–92. 10.5935/0103-507X.20190009
Summary
Keywords
lung transplantation, brain-death donation, circulatory-death donation, interleukin, cytokine storm
Citation
Sandiumenge A, Bello I, Coll-Torres E, Gomez-Brey A, Franco-Jarava C, Miñambres E, Pérez-Redondo M, Mosteiro F, Sánchez-Moreno L, Crowley S, Fieira E, Suberviola B, Mazo CA, Agustí A and Pont T (2024) Systemic Inflammation Differences in Brain-vs. Circulatory-Dead Donors: Impact on Lung Transplant Recipients. Transpl Int 37:12512. doi: 10.3389/ti.2024.12512
Received
04 December 2023
Accepted
17 May 2024
Published
03 June 2024
Volume
37 - 2024
Updates
Copyright
© 2024 Sandiumenge, Bello, Coll-Torres, Gomez-Brey, Franco-Jarava, Miñambres, Pérez-Redondo, Mosteiro, Sánchez-Moreno, Crowley, Fieira, Suberviola, Mazo, Agustí and Pont.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Irene Bello, ibello@clinic.cat
† ORCID: Irene Bello, orcid.org/0000-0002-8188-2361
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.