 Sébastien Tanaka1,2*†
Sébastien Tanaka1,2*† Christian De Tymowski1,3†
Christian De Tymowski1,3† Alexy Tran-Dinh1,4,5Olivier Meilhac2,6Brice Lortat-Jacob1Nathalie Zappella1Sylvain Jean-Baptiste1Tiphaine Robert7Tiphaine Goletto8Cendrine Godet8,9Yves Castier4,5,10Hervé Mal4,8,9
Alexy Tran-Dinh1,4,5Olivier Meilhac2,6Brice Lortat-Jacob1Nathalie Zappella1Sylvain Jean-Baptiste1Tiphaine Robert7Tiphaine Goletto8Cendrine Godet8,9Yves Castier4,5,10Hervé Mal4,8,9 Pierre Mordant4,5,10
Pierre Mordant4,5,10 Enora Atchade1
Enora Atchade1 Jonathan Messika4,8,9,11
Jonathan Messika4,8,9,11 Philippe Montravers1,4,9 and the Bichat Lung Transplant Group‡
Philippe Montravers1,4,9 and the Bichat Lung Transplant Group‡- 1Department of Anesthesiology and Critical Care Medicine, Assistance Publique—Hôpitaux de Paris (AP-HP), Bichat-Claude Bernard Hospital, Paris, France
- 2French Institute of Health and Medical Research (INSERM), U1188 Diabetes Atherothrombosis Réunion Indian Ocean (DéTROI), CYROI Platform, Réunion Island University, Saint-Denis de La Réunion, France
- 3French Institute of Health and Medical Research (INSERM) U1149, Center for Research on Inflammation, Paris, France
- 4UFR Paris Nord, Université Paris Cité, Paris, France
- 5Laboratory for Vascular Translational Science, French Institute of Health and Medical Research (INSERM) U1148, Paris, France
- 6Reunion Island University-Affiliated Hospital, Saint-Denis, France
- 7Department of Biochemistry, Assistance Publique—Hôpitaux de Paris (AP-HP), Bichat-Claude Bernard Hospital, Paris, France
- 8Department of Pneumology and Lung Transplantation, Assistance Publique—Hôpitaux de Paris (AP-HP), Bichat-Claude Bernard Hospital, Paris, France
- 9PHERE, Physiopathology and Epidemiology of Respiratory Diseases, French Institute of Health and Medical Research (INSERM) U1152, Paris, France
- 10Department of Vascular and Thoracic Surgery, Assistance Publique—Hôpitaux de Paris (AP-HP), Bichat-Claude Bernard Hospital, Paris, France
- 11Paris Transplant Group, Paris, France
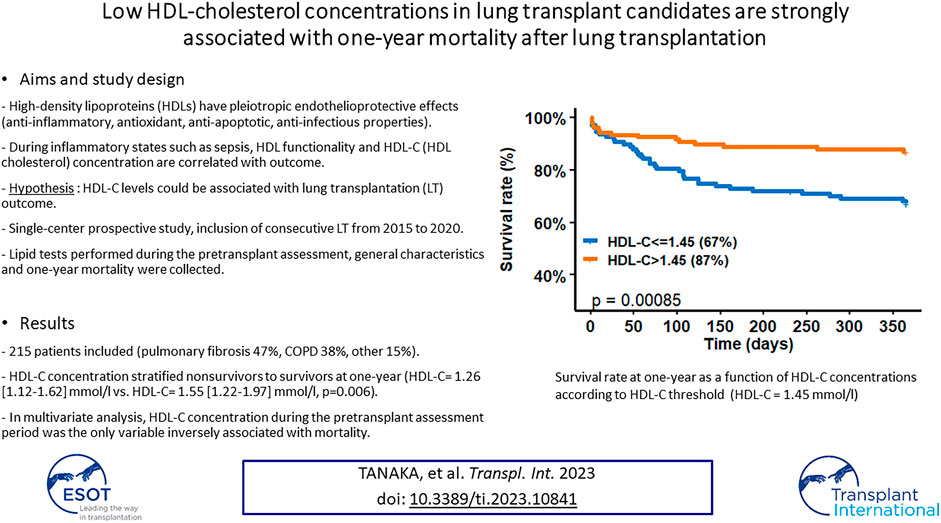
High-density lipoproteins (HDLs), whose main role is the reverse transport of cholesterol, also have pleiotropic anti-inflammatory, antioxidant, anti-apoptotic and anti-infectious properties. During sepsis, HDL cholesterol (HDL-C) concentration is low, HDL particle functionality is altered, and these modifications are correlated with poor outcomes. Based on the protective effects of HDL, we hypothesized that HDL-C levels could be associated with lung transplantation (LT) outcome. We thus looked for an association between basal HDL-C concentration and one-year mortality after LT. In this single-center prospective study including consecutive LTs from 2015 to 2020, 215 patients were included, essentially pulmonary fibrosis (47%) and chronic obstructive pulmonary disease (COPD) (38%) patients. Mortality rate at one-year was 23%. Basal HDL-C concentration stratified nonsurvivors to survivors at one-year (HDL-C = 1.26 [1.12–1.62] mmol/L vs. HDL-C = 1.55 [1.22–1.97] mmol/L, p = 0.006). Multivariate analysis confirmed that HDL-C concentration during the pretransplant assessment period was the only variable inversely associated with mortality. Moreover, mortality at one-year in patients with HDL-C concentrations ≤1.45 mmol/L was significantly higher (log-rank test, p = 0.00085). In conclusion, low basal HDL-C concentrations in candidates for LT are strongly associated with mortality after LT. To better understand this association, further studies in this field are essential and, in particular, a better characterization of HDL particles seems necessary.
Introduction
High-density lipoproteins (HDLs) belong to a family of nanoparticles whose main role is the reverse transport of cholesterol from tissues back to the liver (1). A high concentration of HDL-cholesterol (HDL-C) is negatively correlated with the occurrence of acute cardiovascular events such as ischemic stroke or acute coronary syndrome, conferring to this important scavenger role a strong endothelioprotective function (2, 3). Moreover, HDLs have pleiotropic properties that could play a protective role during acute inflammatory states, such as anti-inflammatory, antioxidant, anti-apoptotic and anti-infectious effects (4–7). For example, during sepsis, it has been shown that the HDL-C concentration is low, but HDL particle functionality is also altered, which could potentially impair endothelioprotective function (8–12). During sepsis, these quantitative and qualitative shifts in HDL are highly associated with morbidity and mortality (7–13).
In contrast with atherosclerosis or sepsis, the problematic lipoprotein and lipid levels in the specific case of lung transplantation (LT) have been less studied. Cottini et al. have shown that a low concentration of HDL-C was associated with more primary graft dysfunction (PGD) after LT (14). Moreover, in a retrospective study involving 172 consecutive LT, the same team demonstrated that the total cholesterol (TC)/HDL-C ratio was associated with mortality after LT (15).
The goal of the present study was to assess the lipid profile, particularly the HDL-C levels, in lung transplant candidates in our LT center and to determine a potential relationship with mortality after LT.
Materials and Methods
Study Population
All consecutive patients who underwent LT at Bichat-Claude Bernard Hospital, Paris, from January 2015 to December 2020 were prospectively included in this observational, single-center analysis. As lipoprotein concentrations may be affected by liver dysfunction, patients scheduled for liver-lung transplantation were excluded from this study.
According to French law, the patient’s absence of refusal was obtained before inclusion in the study. The Paris-North-Hospitals Institutional Review Board (Paris Diderot University, APHP, IRB No. 0006477) reviewed and approved the study.
Objectives
The main objective of this study was to investigate any potential association between the basal value of HDL-C and 1-year mortality. The secondary objectives were to assess the association between the basal value of HDL-C and 1-year mortality among patients with chronic obstructive pulmonary disease (COPD) and fibrosis, the two specific subgroups of our population.
Perioperative Management
The selection of lung transplant candidates (16) and perioperative care (17–20) was standardized for all patients according to current practices. During the intraoperative period, haemodynamic status was monitored using invasive arterial blood pressure, central venous and Swan Ganz catheters, and trans-oesophageal echocardiography. A venoarterial ECMO was implemented in cases of severe pulmonary arterial hypertension, SaO2 <85%, SvO2 <60%, cardiac output<1.5 L/min/m2 when clamping the pulmonary artery, if the patient did not tolerate single-lung ventilation (hypoxemia or hypercapnia), or in case of respiratory failure after transplantation of the first lung. After the surgical procedure, all patients were managed in a single intensive care unit (ICU). Care in ICU are performed according to international recommendations (21).
Data Collection
Demographic characteristics during the pretransplant assessment period were prospectively recorded. Mortality at 1 year was also prospectively collected. Occurrence of primary graft dysfunction (PGD), duration of vasopressor agent administration, need of per or postoperative ECMO support, acute kidney injury (AKI), occurrence of digestive complications such as acute mesenteric ischemia (AMI), duration of mechanical ventilation or length of stay in ICU were also collected. Simplified Acute Physiology Score II (SAPS-II) and sepsis-related organ failure assessment (SOFA) score were registered.
Lipid tests were performed during the pretransplant assessment period in the Biochemistry Laboratory of Bichat Claude-Bernard Hospital. This lipid assessment was performed in stable patients without any acute infectious episode. Total cholesterol (TC), HDL-C, LDL-C and triglyceride concentrations were determined by routine enzymatic assays (CHOL, HDLC, LDLC and TRIG methods, Dimension VISTA System, Siemens Healthineers). The reference values for these assays were HDL-C: >1.40 mmol/L; total cholesterol (TC): 4.40 < N < 5.20 mmol/L and triglycerides: 0.50 < N < 1.7 mmol/L. According to the European Society of Cardiology 2016 recommendations, LDL-C concentration targets have been established depending on vascular risk factors (22). All measurement methods were carried out in accordance with the guidelines.
Statistical Analysis
Continuous variables are expressed as medians with interquartile ranges (IQRs) and were compared with the Mann–Whitney U test. Categorical variables are expressed as counts and percentages and were compared with Fisher’s exact test or the chi-square test, as appropriate. For 1-year mortality discrimination, receiver operating characteristic curve (ROC) analysis was performed, and the area under the curve (AUC) was calculated. The Youden index was used to determine the best threshold value of HDL-C.
Time-to-event analyses were estimated with Kaplan–Meier analyses. Multivariate associations were computed with binary logistic regression models; variables with nominal 2-tailed p values less than 0.2 were entered into the multivariate model, except for variables with obvious collinearity. The final models were selected using backward stepwise regression based on the Akaike information criterion (AIC). All statistical analyses were performed using R statistical software (https://www.r-project.org/). A p-value <0.05 was considered statistically significant.
Results
Whole Population
General Characteristics
Between January 2015 and December 2020, 269 patients underwent LT in our institution. Three patients planned for liver-lung transplantation were excluded from the analysis. Fifty-one patients were excluded from the analysis because their lipid profile was not determined or was incomplete. Overall, 215 patients were finally included in this study. A total of 149 patients (69%) underwent double LT. The patient’s general characteristics during the pretransplant assessment period are presented in Table 1. In this cohort, 10 (4.7%) patients had chronic coronary disease and all these patients underwent a percutaneous coronary intervention. No patient required coronary artery bypass graft (CABG). Moreover, only 10 (4.7%) patients had significant aortic and peripheral vascular calcifications. There was no difference in general characteristics between alive and deceased patients at 1 year.
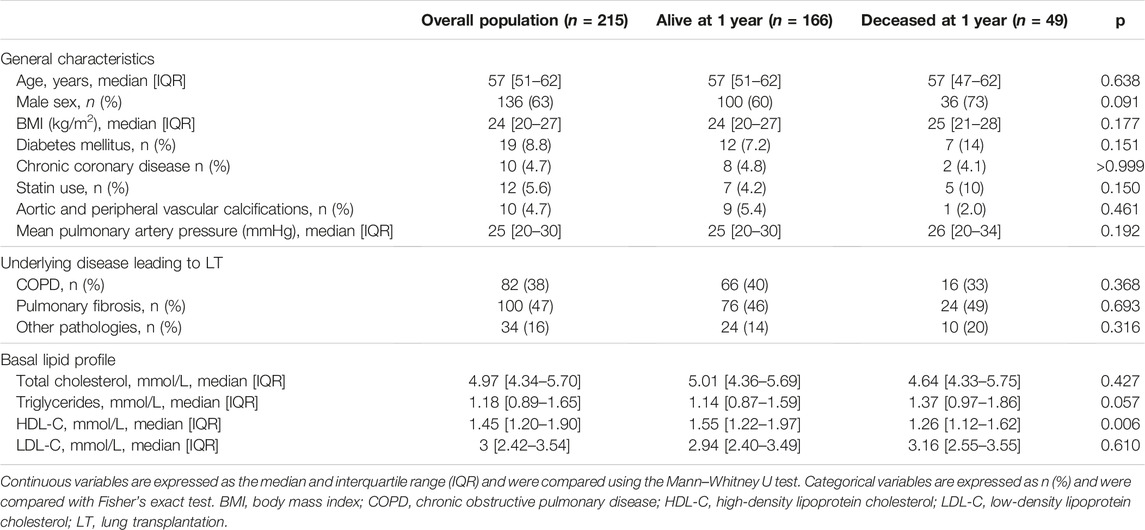
TABLE 1. General characteristics, underlying disease and lipid profile of the overall population stratified by mortality at 1 year.
Blood Lipid Profile
The median delay between the lipid test and LT was 303 [170–552] days. Table 1 presents the lipid profile in the overall population. A comparison between patients alive or deceased at 1 year is also given. In the entire population, the median lipid concentrations were normal, according to the standard values (22). There was no difference between TC, LDL-C and TG concentrations between deceased and alive patients at 1 year. Interestingly, non-survivors had a lower HDL-C concentration than survivors at 1 year (HDL-C = 1.26 [1.12–1.62] mmol/L vs. HDL-C = 1.55 [1.22–1.97] mmol/L, p = 0.006).
Moreover, whereas there was no difference in mortality rates at 1 year between patients with and without chronic coronary disease (p > 0.999), HDL-C concentrations in patients with chronic coronary disease were lower than in patients without (HDL-C = 1.18 [1.02, 1.30] mmol/L vs. 1.50 [1.21, 1.96] mmol/L, p = 0.008). There was no difference in HDL-C concentrations when comparing patients with and without aortic and peripheral vascular calcifications (HDL-C = 1.69 [1.33, 2.30] mmol/L vs. 1.45 [1.20, 1.87] mmol/L, p = 0.138).
Outcome
The mortality rate at 1 year was 23%. Multivariate analysis with general characteristics during the pretransplant assessment period was performed. These results are expressed in Table 2. A high basal HDL concentration was predictive of good outcomes, suggesting a significant protective effect for 1-year mortality (odds ratio 0.35, 95% CI [0.15, 0.75], p = 0.008).

TABLE 2. Multivariate analysis of risk factors for mortality at 1 year.
ROC curves were generated to assess the ability of lipid profiles (TC, HDL-C, LDL-C and TG) to discriminate 1-year mortality (Supplementary Figure S1). HDL-C had a higher AUC [0.63 (95% CI 0.54–0.71)]. The best threshold value of HDL-C was 1.45 mmol/L (Youden index, sensitivity = 0.71, specificity = 0.56, positive predictive value (PPV) = 0.32, negative predictive value (NPV) = 0.86).
Figure 1 shows the survival rate at 1 year as a function of HDL-C concentrations according to the HDL-C threshold (HDL-C = 1.45 mmol/L). Survival at 1 year of patients with HDL-C concentrations ≤1.45 mmol/L was significantly lower (log-rank test, p = 0.00085).
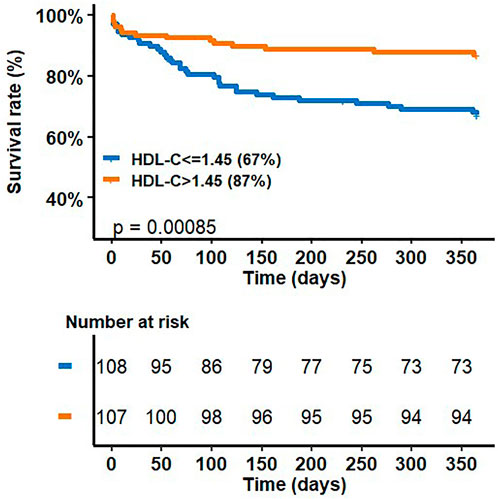
FIGURE 1. survival rate at 1 year as a function of HDL-C concentrations according to HDL-C threshold (HDL-C = 1.45 mmol/L).
Supplementary Table S1 shows the different values of outcome variables at 1-year mortality.
Subgroup of COPD Patients
- Supplementary Table S2 describes the univariate and multivariate analysis of the general characteristics and lipid profile during the pretransplant assessment period and mortality at 1 year in the subgroup of COPD patients. As in the whole population, a high basal HDL-C concentration predicted a good outcome at 1 year in the subgroup of COPD patients (odds ratio 0.13, 95% CI [0.03–0.49], p = 0.004).
- ROC curves were constructed to assess the ability of lipid profiles (TC, HDL-C, LDL-C and TG) to discriminate 1-year mortality in the subgroup of COPD patients (Supplementary Figure S2A). HDL-C had a higher AUC [0.76 (95% CI 0.65–0.82)]. The best threshold value of HDL-C was 1.45 mmol/L (Youden index, sensitivity = 0.75, specificity = 0.76, positive predictive value (PPV) = 0.43, negative predictive value (NPV) = 0.93).
- Figure 2A shows the survival rate at 1 year as a function of HDL-C concentrations according to the HDL-C threshold (HDL-C = 1.45 mmol/L). The survival rate at 1 year of patients with HDL-C concentrations ≤1.45 mmol/L was significantly lower (log-rank test, p < 0.0001).
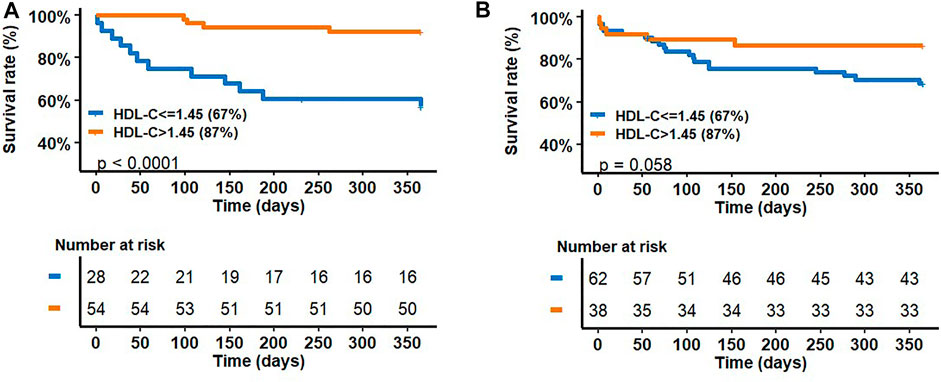
FIGURE 2. survival rate at 1-year as a function of HDL-C concentrations according to HDL-C threshold (HDL-C = 1.45 mmol/L) in the COPD (A) and in fibrosis (B) sub-groups.
Subgroup of Patients With Fibrosis
- Supplementary Table S3 shows univariate and multivariate analyses of the general characteristics during the pretransplant assessment period and the mortality at 1 year in the subgroup of fibrosis patients. Interestingly, in multivariate analysis, a high TG concentration was significantly associated with 1-year mortality (odds ratio 1.96, 95% CI [1.02–3.85], p = 0.044). No relationship between HDL-C concentration and mortality was found.
- ROC curves were generated to assess the ability of lipid profiles (TC, HDL-C, LDL-C and TG) to discriminate 1-year mortality in the subgroup of fibrosis patients (Supplementary Figure S2B). All lipid and lipoprotein values had low AUCs.
- Figure 2B shows the survival rate at 1 year as a function of HDL-C concentrations according to the HDL-C threshold (HDL-C = 1.45 mmol/L). There was no significant difference between survivors and non-survivors patients according to the HDL-C threshold (log-rank test, p = 0.058).
Discussion
The main message of this manuscript is that low basal HDL-C concentration assessed during the pretransplant period is strongly associated with 1-year mortality after LT.
To our knowledge, our study is the first to show this link. Only one previous study has looked at the relationship between the lipid profile and mortality in the context of LT (15). Wenger et al., in a population of 144 LT patients, described a relationship between low basal HDL-C concentration and the occurrence of major cardiovascular events, but did not find any relationship with mortality (15). However, these authors showed that patients who died had a significantly higher TC/HDL-C ratio.
Unlike atherosclerosis or sepsis, where both HDL-C concentration and HDL particle functionality have been extensively studied (8–25), only a few studies have reported HDL-C levels in the context of respiratory disease and LT (26). A retrospective analysis of 126 consecutive individuals evaluated for LT with a diagnosis of COPD showed that HDL-C levels were increased and this was partially attributable to oral steroid use (27). Interestingly, in this study, the HDL-C concentration was not associated with a reduced risk of coronary artery disease. This same team demonstrated that LT in COPD patients led to reductions in the serum levels of HDL-C (28). Moreover, when compared with other populations and, in particular, patients with fibrosis, the HDL-C concentration in COPD patients is very discriminating, which indirectly raises questions about the specific basal metabolism of this population when they are evaluated for LT.
Furthermore, in 69 patients with pulmonary arterial hypertension (PAH), a previous study reported that their HDL-C levels were significantly decreased and were associated with poor clinical outcomes independent of cardiovascular risk factors, insulin resistance and the severity of PAH (29). In patients with idiopathic pulmonary fibrosis (IPF), reduced amounts of apolipoprotein A-I, the major apolipoprotein comprising HDL particles, have been found in bronchoalveolar lavage fluid compared to normal controls (30). Interestingly, the data in our population of fibrosis patients did not highlight an association between basal HDL-C and mortality. The complexity of the fibrosis entity, sometimes occurring in relationship with systemic diseases, may explain, at least partially, the lack of associations. Barochia et al. showed in a study using nuclear magnetic resonance spectroscopy that high levels of small HDL particles (i.e., more functional HDL particles) were negatively correlated with lower mortality or LT (31). Beyond a modification of HDL-C concentration, structural changes of the particles may then influence the outcome.
Since our study was purely exploratory, our observations are only assumptions and it is thus impossible to conclude why we found a strong link between basal HDL-C concentrations and mortality. In light of our results, HDL-C appears to be a marker or an effector in the survival.
Nevertheless, during the per/postoperative periods of LT, acute inflammatory episodes are frequently described, such as systemic inflammatory response syndrome as well as sepsis (19–35). It has been reported that during these states, there is both a decrease in HDL-C and a functional modification of HDL particles with, in particular, a proinflammatory profile (11–42). Importantly, these shifts are associated with poor outcomes. Therefore, if the HDL-C concentration is low under basal conditions and there are both qualitative and quantitative changes during and after LT, the poor prognosis of patients can then be understood.
Our results motivate more powerful clinical studies and experimental studies: If clinical studies confirmed our result, the basal HDL-C concentration could be proposed for discriminating transplant candidates. Moreover, the functionalities of HDL particles before/during/after LT probably deserve additional investigation. Whereas during sepsis, functional and structural changes have been well described (7), no study has yet investigated these functionalities in LT. Studies, in particular -omics analyses, seem necessary to better characterize these LT candidates.
Our study has several limitations:
First, this investigation being purely observational, we have no element that can rationally explain our results. Second, the monocentric nature of our work with only 215 patients is a limitation, which can lead to recruitment bias. Third, the mixture of varied respiratory pathologies (COPD and fibrosis) can also bring about some biases. A focus on the specific COPD candidates could be very informative. Fourth, an analysis of HDL-C concentrations per and postoperatively would have been informative. Fifth, even if 1-year mortality is not a reliable indicator of LT transplant center performance (43), our mortality rate at 1 year (23%) seems to be slightly high and this could induce some bias. The high proportion of fibrosis and high emergency LT (18%) could possibly explain this elevated rate. Finally, whereas there was no difference in mortality rates at 1-year between patients with and without chronic coronary disease, HDL-C concentration in patients with chronic coronary disease were lower than in patients without. Even if this population is very small (n = 10), it could induce a bias.
In conclusion, our work showed that a low basal HDL-C concentration in candidates for LT was associated with increased mortality after LT. HDL-C appears to be a marker or an effector in the survival. To better understand this association, additional and more powerful studies are required. A better characterization of HDL particles is also a huge challenge.
Investigators of the Bichat Lung Transplant Group
Agnès Abadie, Enora Atchade, Mouna Ben-rehouma, Vincent Bunel, Yves Castier, Pierre Cerceau, Diego Ferreira, Gwenn Frere, Lucie Genet, Cendrine Godet, Tiphaine Goletto, Sylvain Jean-Baptiste, Gilles Jebrak, Elie Kantor, Paul Labed, Dan Longrois, Brice Lortat-Jacob, Hervé Mal, Armelle Marceau, Chahine Medraoui, Charlotte Thibaut de Menonville, Jonathan Messika, Alexandre Mignon, Domitille Mouren, Quentin Pellenc, Régis Renard, Arnaud Roussel, Mathilde Salpin, Léa Copelovici, Sandrine Boudinet, Alice Savary, Jean Senemaud, Aurélie Snauwert, Jules Stern, Sebastien Tanaka, Parvine Tashk, Sandrine Tissot, Alexy Tran-Dinh, Sabrina Trigueiros, Christian de Tymowski, Gaëlle Weisenburger, Nathalie Zappella.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics Statement
According to French law, the patient’s absence of refusal was obtained before inclusion in the study. The Paris-North-Hospitals Institutional Review Board (Paris Diderot University, APHP, IRB No. 0006477) reviewed and approved the study.
Author Contributions
ST, CT, OM, and PhM contributed to study concept and design. ST and CT performed statistical analysis. ST, CT, AT-D, OM, BL-J, NZ, SJ-B, TR, TG, CG, YC, HM, PiM, EA, JM, and PhM were involved in data analysis and interpretation. ST, CT, OM, JM, PiM, AT-D, CG, EA, and PhM performed critical revision of the manuscript. All the authors read and approved the final manuscript.
Conflict of Interest
CG reports having received grant support from Ohre Pharma, Pfizer, MSD, SOS Oxygène, ISIS Medical, Vivisol, Elivie and AstraZeneca, speaker fees, travel support from Pfizer, MSD and speaker fees for board memberships from SOS Oxygène and Pulmatrix. JM received congress reimbursement fees from Biotest and CSL Behring, Fingers Xed.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We warmly thank the medical and paramedical teams of Vascular and Thoracic Surgery, Pneumology, Anesthesiology and surgical ICU departments of the Bichat Hospital, Paris, France.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontierspartnerships.org/articles/10.3389/ti.2023.10841/full#supplementary-material
Abbreviations
AIC, akaike information criterion; AUC, area under the curve; COPD, chronic obstructive pulmonary disease; HDL, high-density lipoprotein; HDL-C, HDL cholesterol; ICU, intensive care unit; LDL, low-density lipoprotein; LDL-C, LDL cholesterol; LT, lung transplantation; NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic; TC, total cholesterol; TG, triglyceride.
References
1. Nofer, JR, Levkau, B, Wolinska, I, Junker, R, Fobker, M, von Eckardstein, A, et al. Suppression of Endothelial Cell Apoptosis by High Density Lipoproteins (HDL) and HDL-Associated Lysosphingolipids. J Biol Chem (2001) 276(37):34480–5. doi:10.1074/jbc.M103782200
2. Wilson, PW, Abbott, RD, and Castelli, WP. High Density Lipoprotein Cholesterol and Mortality. The Framingham Heart Study. Framingham Heart Study Arteriosclerosis Déc (1988) 8(6):737–41. doi:10.1161/01.atv.8.6.737
3. Cooney, MT, Dudina, A, De Bacquer, D, Wilhelmsen, L, Sans, S, Menotti, A, et al. HDL Cholesterol Protects against Cardiovascular Disease in Both Genders, at All Ages and at All Levels of Risk. Atheroscler oct (2009) 206(2):611–6. doi:10.1016/j.atherosclerosis.2009.02.041
4. Pirillo, A, Catapano, AL, and Norata, GD. HDL in Infectious Diseases and Sepsis. Handb Exp Pharmacol (2015) 224:483–508. doi:10.1007/978-3-319-09665-0_15
5. Tran-Dinh, A, Diallo, D, Delbosc, S, Varela-Perez, LM, Dang, QB, Lapergue, B, et al. HDL and Endothelial protection. Br J Pharmacol Juin (2013) 169(3):493–511. doi:10.1111/bph.12174
6. Ulevitch, RJ, Johnston, AR, and Weinstein, DB. New Function for High Density Lipoproteins. Their Participation in Intravascular Reactions of Bacterial Lipopolysaccharides. J Clin Invest Nov (1979) 64(5):1516–24. doi:10.1172/JCI109610
7. Tanaka, S, Couret, D, Tran-Dinh, A, Duranteau, J, Montravers, P, Schwendeman, A, et al. High-density Lipoproteins during Sepsis: from Bench to Bedside. Crit Care (2020) 24(1):134. doi:10.1186/s13054-020-02860-3
8. Chien, JY, Jerng, JS, Yu, CJ, and Yang, PC. Low Serum Level of High-Density Lipoprotein Cholesterol Is a Poor Prognostic Factor for Severe Sepsis. Crit Care Med (2005) 33(8):1688–93. doi:10.1097/01.ccm.0000171183.79525.6b
9. Barlage, S, Gnewuch, C, Liebisch, G, Wolf, Z, Audebert, FX, Gluck, T, et al. Changes in HDL-Associated Apolipoproteins Relate to Mortality in Human Sepsis and Correlate to Monocyte and Platelet Activation. Intensive Care Med (2009) 35(11):1877–85. doi:10.1007/s00134-009-1609-y
10. Tanaka, S, Stern, J, Bouzid, D, Robert, T, Dehoux, M, Snauwaert, A, et al. Relationship between Lipoprotein Concentrations and Short-Term and 1-year Mortality in Intensive Care Unit Septic Patients: Results from the HIGHSEPS Study. Ann Intensive Care (2021) 11(1):11. doi:10.1186/s13613-021-00800-0
11. Tanaka, S, Diallo, D, Delbosc, S, Genève, C, Zappella, N, Yong-Sang, J, et al. High-density Lipoprotein (HDL) Particle Size and Concentration Changes in Septic Shock Patients. Ann Intensive Care (2019) 9(1):68. doi:10.1186/s13613-019-0541-8
12. Sharma, NK, Tashima, AK, Brunialti, MKC, Ferreira, ER, Torquato, RJS, Mortara, RA, et al. Proteomic Study Revealed Cellular Assembly and Lipid Metabolism Dysregulation in Sepsis Secondary to Community-Acquired Pneumonia. Sci Rep (2017) 7(1):15606. doi:10.1038/s41598-017-15755-1
13. Tanaka, S, Labreuche, J, Drumez, E, Harrois, A, Hamada, S, Vigué, B, et al. Low HDL Levels in Sepsis versus Trauma Patients in Intensive Care Unit. Ann Intensive Care Déc (2017) 7(1):60. doi:10.1186/s13613-017-0284-3
14. Cottini, SR, Ehlers, UE, Pagnamenta, A, Brandi, G, Weder, W, Schuepbach, RA, et al. Pretransplant Dyslipidaemia Influences Primary Graft Dysfunction after Lung Transplantation. Interact Cardiovasc Thorac Surg Avr (2016) 22(4):402–5. doi:10.1093/icvts/ivv295
15. Wenger, U, Cottini, SR, Noll, G, Arndt, S, Stehberger, PA, Klinzing, S, et al. Pretransplant Dyslipidaemia Determines Outcome in Lung Transplant Recipients. Lipids Health Dis. 23 avr 2013;12:53, doi:10.1186/1476-511X-12-53
16. Leard, LE, Holm, AM, Valapour, M, Glanville, AR, Attawar, S, Aversa, M, et al. Consensus Document for the Selection of Lung Transplant Candidates: An Update from the International Society for Heart and Lung Transplantation. J Heart Lung Transpl nov (2021) 40(11):1349–79. doi:10.1016/j.healun.2021.07.005
17. Elmaleh, Y, De Tymowski, C, Zappella, N, Jean-Baptiste, S, Tran-Dinh, A, Tanaka, S, et al. Blood Transfusion of the Donor Is Associated with Stage 3 Primary Graft Dysfunction after Lung Transplantation. Clin Transpl sept (2021) 35(9):e14407. doi:10.1111/ctr.14407
18. Atchade, E, Younsi, M, Elmaleh, Y, Tran-Dinh, A, Jean-Baptiste, S, Tanaka, S, et al. Intensive Care Readmissions in the First Year after Lung Transplantation: Incidence, Early Risk Factors and Outcome. Anaesth Crit Care Pain Med Déc (2021) 40(6):100948. doi:10.1016/j.accpm.2021.100948
19. Tanaka, S, Geneve, C, Tebano, G, Grall, N, Piednoir, P, Bronchard, R, et al. Morbidity and Mortality Related to Pneumonia and TRACHEOBRONCHITIS in ICU after Lung Transplantation. BMC Pulm Med (2018) 18(1):43. doi:10.1186/s12890-018-0605-9
20. Kao, CC, and Parulekar, AD. Postoperative Management of Lung Transplant Recipients. J Thorac Dis Sept (2019) 11(14):S1782–S1788. doi:10.21037/jtd.2019.05.60
21. Marczin, N, de Waal, EEC, Hopkins, PMA, Mulligan, MS, Simon, A, Shaw, AD, et al. International Consensus Recommendations for Anesthetic and Intensive Care Management of Lung Transplantation. An EACTAIC, SCA, ISHLT, ESOT, ESTS, and AST Approved Document. J Heart Lung Transpl nov (2021) 40(11):1327–48. doi:10.1016/j.healun.2021.07.012
22. Catapano, AL, Graham, I, De Backer, G, Wiklund, O, Chapman, MJ, Drexel, H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur Heart J (2016) 1437(39):2999–3058. doi:10.1093/eurheartj/ehw272
23. Abbott, RD, Garrison, RJ, Wilson, PW, Epstein, FH, Castelli, WP, Feinleib, M, et al. Joint Distribution of Lipoprotein Cholesterol Classes. The Framingham Study. Framingham Study Arteriosclerosis Juin (1983) 3(3):260–72. doi:10.1161/01.atv.3.3.260
24. Rohatgi, A, Khera, A, Berry, JD, Givens, EG, Ayers, CR, Wedin, KE, et al. HDL Cholesterol Efflux Capacity and Incident Cardiovascular Events. N Engl J Med (2014) 371(25):2383–93. doi:10.1056/NEJMoa1409065
25. Vaisar, T, Pennathur, S, Green, PS, Gharib, SA, Hoofnagle, AN, Cheung, MC, et al. Shotgun Proteomics Implicates Protease Inhibition and Complement Activation in the Antiinflammatory Properties of HDL. J Clin Invest Mars (2007) 117(3):746–56. doi:10.1172/JCI26206
26. Gordon, EM, Figueroa, DM, Barochia, AV, Yao, X, and Levine, SJ. High-density Lipoproteins and Apolipoprotein A-I: Potential New Players in the Prevention and Treatment of Lung Disease. Front Pharmacol (2016) 7:323. doi:10.3389/fphar.2016.00323
27. Reed, RM, Iacono, A, DeFilippis, A, Eberlein, M, Girgis, RE, and Jones, S. Advanced Chronic Obstructive Pulmonary Disease Is Associated with High Levels of High-Density Lipoprotein Cholesterol. J Heart Lung Transpl juin (2011) 30(6):674–8. doi:10.1016/j.healun.2010.12.010
28. Reed, RM, Hashmi, S, Eberlein, M, Iacono, A, Netzer, G, DeFilippis, A, et al. Impact of Lung Transplantation on Serum Lipids in COPD. Respir Med Déc (2011) 105(12):1961–8. doi:10.1016/j.rmed.2011.10.003
29. Heresi, GA, Aytekin, M, Newman, J, DiDonato, J, and Dweik, RA. Plasma Levels of High-Density Lipoprotein Cholesterol and Outcomes in Pulmonary Arterial Hypertension. Am J Respir Crit Care Med (2010) 182(5):661–8. doi:10.1164/rccm.201001-0007OC
30. Kim, TH, Lee, YH, Kim, KH, Lee, SH, Cha, JY, Shin, EK, et al. Role of Lung Apolipoprotein A-I in Idiopathic Pulmonary Fibrosis: Antiinflammatory and Antifibrotic Effect on Experimental Lung Injury and Fibrosis. Am J Respir Crit Care Med (2010) 182(5):633–42. doi:10.1164/rccm.200905-0659OC
31. Barochia, AV, Kaler, M, Weir, N, Gordon, EM, Figueroa, DM, Yao, X, et al. Serum Levels of Small HDL Particles Are Negatively Correlated with Death or Lung Transplantation in an Observational Study of Idiopathic Pulmonary Fibrosis. Eur Respir J Déc (2021) 58(6):2004053. doi:10.1183/13993003.04053-2020
32. Meilhac, O, Tanaka, S, and Couret, D. High-Density Lipoproteins Are Bug Scavengers. Biomolecules. (2020) 10(4):598. doi:10.3390/biom10040598
33. Pietrantoni, C, Minai, OA, Yu, NC, Maurer, JR, Haug, MT, Mehta, AC, et al. Respiratory Failure and Sepsis Are the Major Causes of ICU Admissions and Mortality in Survivors of Lung Transplants. Chest Févr (2003) 123(2):504–9. doi:10.1378/chest.123.2.504
34. Chambers, DC, Perch, M, Zuckermann, A, Cherikh, WS, Harhay, MO, Hayes, D, et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-Eighth Adult Lung Transplantation Report - 2021; Focus on Recipient Characteristics. J Heart Lung Transpl (2021) 40(10):1060–72. doi:10.1016/j.healun.2021.07.021
35. Shepherd, HM, Gauthier, JM, Li, W, Krupnick, AS, Gelman, AE, and Kreisel, D. Innate Immunity in Lung Transplantation. J Heart Lung Transpl juill (2021) 40(7):562–8. doi:10.1016/j.healun.2021.03.017
36. Hacquebard, M, Ducart, A, Schmartz, D, Malaisse, WJ, and Carpentier, YA. Changes in Plasma LDL and HDL Composition in Patients Undergoing Cardiac Surgery. Lipids Déc (2007) 42(12):1143–53. doi:10.1007/s11745-007-3114-9
37. Tanaka, S, De Tymowski, C, Zappella, N, Snauwaert, A, Robert, T, Lortat-Jacob, B, et al. Lipoprotein Concentration in Patients Requiring Extracorporeal Membrane Oxygenation. Sci Rep (2021) 11(1):17225. doi:10.1038/s41598-021-96728-3
38. de la Llera Moya, M, McGillicuddy, FC, Hinkle, CC, Byrne, M, Joshi, MR, Nguyen, V, et al. Inflammation Modulates Human HDL Composition and Function In Vivo. Atheroscler juin (2012) 222(2):390–4. doi:10.1016/j.atherosclerosis.2012.02.032
39. Vaisar, T, Tang, C, Babenko, I, Hutchins, P, Wimberger, J, Suffredini, AF, et al. Inflammatory Remodeling of the HDL Proteome Impairs Cholesterol Efflux Capacity. J Lipid Res Août (2015) 56(8):1519–30. doi:10.1194/jlr.M059089
40. Tanaka, S, De Tymowski, C, Assadi, M, Zappella, N, Jean-Baptiste, S, Robert, T, et al. Lipoprotein Concentrations over Time in the Intensive Care Unit COVID-19 Patients: Results from the ApoCOVID Study. PLoS One (2020) 15(9):e0239573. doi:10.1371/journal.pone.0239573
41. Begue, F, Tanaka, S, Mouktadi, Z, Rondeau, P, Veeren, B, Diotel, N, et al. Altered High-Density Lipoprotein Composition and Functions during Severe COVID-19. Sci Rep (2021) 11(1):2291. doi:10.1038/s41598-021-81638-1
42. Sharma, NK, Ferreira, BL, Tashima, AK, Brunialti, MKC, Torquato, RJS, Bafi, A, et al. Lipid Metabolism Impairment in Patients with Sepsis Secondary to Hospital Acquired Pneumonia, a Proteomic Analysis. Clin Proteomics (2019) 16:29. doi:10.1186/s12014-019-9252-2
Keywords: mortality, lung transplantation, outcome, HDL-cholesterol, lipoprotein
Citation: Tanaka S, Tymowski CD, Tran-Dinh A, Meilhac O, Lortat-Jacob B, Zappella N, Jean-Baptiste S, Robert T, Goletto T, Godet C, Castier Y, Mal H, Mordant P, Atchade E, Messika J, Montravers P and the Bichat Lung Transplant Group (2023) Low HDL-Cholesterol Concentrations in Lung Transplant Candidates are Strongly Associated With One-Year Mortality After Lung Transplantation. Transpl Int 36:10841. doi: 10.3389/ti.2023.10841
Received: 17 August 2022; Accepted: 03 January 2023;
Published: 16 January 2023.
Copyright © 2023 Tanaka, Tymowski, Tran-Dinh, Meilhac, Lortat-Jacob, Zappella, Jean-Baptiste, Robert, Goletto, Godet, Castier, Mal, Mordant, Atchade, Messika, Montravers and the Bichat Lung Transplant Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sébastien Tanaka, c2ViYXN0aWVuLnRhbmFrYUBhcGhwLmZy
†These authors have contributed equally to this work
‡Bichat Lung Transplant Group members are listed at the end of the paper