 Maarten Naesens1*
Maarten Naesens1* Alexandre Loupy2
Alexandre Loupy2 Luuk Hilbrands3
Luuk Hilbrands3 Rainer Oberbauer4
Rainer Oberbauer4 Maria Irene Bellini5Denis Glotz6
Maria Irene Bellini5Denis Glotz6 Josep Grinyó7
Josep Grinyó7 Uwe Heemann8
Uwe Heemann8 Ina Jochmans9
Ina Jochmans9 Liset Pengel10Marlies Reinders11
Liset Pengel10Marlies Reinders11 Stefan Schneeberger12
Stefan Schneeberger12 Klemens Budde13
Klemens Budde13- 1Department of Microbiology, Immunology and Transplantation, KU Leuven, Leuven, Belgium
- 2Paris Translational Research Center for Organ Transplantation, Hôpital Necker, Paris, France
- 3Department of Nephrology, Radboud University Medical Center, Nijmegen, Netherlands
- 4Department of Nephrology and Dialysis, Medical University of Vienna, Vienna, Austria
- 5Department of Surgical Sciences, Sapienza University of Rome, Rome, Italy
- 6Paris Translational Research Center for Organ Transplantation, Hôpital Saint Louis, Paris, France
- 7University of Barcelona, Barcelona, Spain
- 8Department of Nephrology, Technical University of Munich, Munich, Germany
- 9Transplantation Research Group, Department of Microbiology, Immunology and Transplantation, KU Leuven, Leuven, Belgium
- 10Centre for Evidence in Transplantation, Nuffield Department of Surgical Sciences, University of Oxford, Oxford, United Kingdom
- 11Erasmus MC Transplant Institute, Department of Internal Medicine, University Medical Center Rotterdam, Rotterdam, Netherlands
- 12Department of General, Transplant and Thoracic Surgery, Medical University of Innsbruck, Innsbruck, Austria
- 13Department of Nephrology and Medical Intensive Care, Charité Universitätsmedizin Berlin, Berlin, Germany
Conditional marketing authorization (CMA) facilitates timely access to new drugs for illnesses with unmet clinical needs, such as late graft failure after kidney transplantation. Late graft failure remains a serious, burdensome, and life-threatening condition for recipients. This article has been developed from content prepared by members of a working group within the European Society for Organ Transplantation (ESOT) for a Broad Scientific Advice request, submitted by ESOT to the European Medicines Agency (EMA), and reviewed by the EMA in 2020. The article presents the rationale for using surrogate endpoints in clinical trials aiming at improving late graft failure rates, to enable novel kidney transplantation therapies to be considered for CMA and improve access to medicines. The paper also provides background data to illustrate the relationship between primary and surrogate endpoints. Developing surrogate endpoints and a CMA strategy could be particularly beneficial for studies where the use of primary endpoints would yield insufficient statistical power or insufficient indication of long-term benefit following transplantation.
Introduction
The guideline CHMP/EWP/263148/06 of the European Medicines Agency (EMA) Committee for Medicinal Products for Human Use (CHMP), issued in 2008, identifies the primary composite endpoint for clinical trials in organ transplantation as recipient death, graft failure, biopsy-confirmed acute rejection, and graft (dys)function (1). Based on this composite endpoint, specific immunosuppressive drugs have received full (standard) marketing authorization for transplantation. However, CHMP/EWP/263148/06 does not mention any opportunities for other novel drugs to proceed to conditional marketing authorization (CMA), such as drugs that aim to improve long-term outcomes after kidney transplantation. This represents an area of considerable unmet medical need and restricts the development of novel treatments.
The present article proposes the rationale for surrogate endpoints for CMA, for novel kidney transplantation therapies; the paper also provides background data that illustrate the relationship between surrogate and primary endpoints, to support full marketing authorization.
CMA applications based on clinical trials using surrogate endpoints should not replace full marketing authorization applications based on studies using accepted primary endpoints. As discussed elsewhere in this Special Issue, graft rejection is acceptable as a primary endpoint for obtaining full marketing authorization by the EMA, because graft rejection is considered directly clinically meaningful, requiring therapies for rejection (2–4). Kidney function (incidence of end-stage renal disease, proportional decrease in eGFR, and annual decrease in eGFR—slope) is also well accepted by the EMA/CHMP as a primary endpoint to assess efficacy of medicinal products to slow progression of chronic renal insufficiency in chronic kidney disease. CHMP/EMA confirmed that this reasoning can be adopted for trials of kidney transplantation (5).
Rather, the CMA strategy and surrogate endpoints are suggested for studies where use of the accepted primary endpoints would yield insufficient statistical power or insufficient indication of long-term benefit. Applied to novel immunosuppressive agents, long-term benefit for kidney transplantation would equal decreased rates of late graft failure. It is therefore also important to have a very clear definition of late graft failure.
Here, we discuss the definition of late graft failure, and the rationale to consider late graft failure as a disease with unmet clinical need, allowing for CMA applications for novel therapies aimed at improving long-term kidney transplant outcomes. Endpoints that could be considered as surrogates for late graft failure are discussed separately in this Special Issue (6).
Definition of Late Graft Failure
In discussions relating to the present article, we defined overall (all-cause) graft failure as a composite of two important primary endpoints: loss of graft function (i.e., return to dialysis or pre-emptive re-transplantation), and recipient death with a functioning graft.
We consider that using 1 year post transplantation as the border between early and late graft failure reflects current clinical research standards and epidemiological data. These illustrate a fundamental difference in general improvement of graft outcome within and beyond 1 year after transplantation (7).
In addition, a 1-year threshold for the definition of late graft failure could be appropriate, given that research standards usually consider primary endpoints at 6 months to 1 year following transplantation. This was the case for pivotal trials that supported the approval of immunosuppressive drugs (reviewed in (8)). The 1-year threshold for early versus late graft failure also reflects evidence that short-term graft outcomes (i.e, failure within the first year) improve over time (7); this was not the case for long-term graft failure, which was defined as any failure from 1 year post-transplant (7). In addition, in the Collaborative Transplant Study European data analyses (9), the 1-year graft survival rate improved considerably between 1986 and 1999, but no noteworthy improvement was seen for graft survival beyond the first year after transplantation. Lastly, there are relevant differences in the reasons for graft loss in different periods after transplantation; it is not the purpose of the present paper to discuss them (10).
Rationale for CMA Applications for Late Graft Failure
The European Medicines Agency (EMA)-initiated concept of CMA (11) is an important tool for ensuring timely access to medicines in areas of unmet medical need. For CMA application, medicines for human use are eligible if they belong to at least one of the following three categories:
• Aimed at treating, preventing, or diagnosing seriously debilitating or life-threatening diseases
• Intended for use in emergency situations (less-comprehensive pharmaceutical and non-clinical data may also be accepted)
• Designated as orphan medicines, i.e., for the diagnosis, prevention, or treatment of a life-threatening or chronically debilitating condition that is rare (affecting <5 in 10,000 people in the European Union [EU]).
Late Graft Failure: Seriously Debilitating, Life-Threatening
In kidney transplant patient populations, late graft failure is a common, seriously debilitating, and life-threatening condition; no specific measures are available for its prevention. Immunosuppressive drugs were primarily approved for prevention of early acute rejection, with limited impact on (late) graft failure (8). In Europe, death-censored graft failure rates (censoring for death with a functioning graft) beyond the first year post-transplantation have shown some improvement since the late 1980s (7, 9). However, ∼5% of grafts are still lost annually after the first year, including loss due to recipient death (7, 12, 13). On this basis alone, medicines that aim to prevent late kidney graft failure could be proposed for CMA.
Several aspects make late kidney graft failure a serious condition for which there is an unmet medical need. First, there is the requirement for dialysis reinitiation, which carries a heightened risk of mortality, comorbidities, and impaired health-related quality of life. Second, there is a high risk of human leukocyte antigen antibody (HLA) sensitization, which is associated with prolonged waiting time for repeat transplantation and further increased risk of dialysis complications. Third, increased risk of graft failure is observed after re-transplantation, which is related to heightened risk of antibody-mediated rejection (AMR) because of preformed antibodies against the first donor kidney (13, 14). In addition, increased morbidity and inferior outcomes after re-transplantation can result from diverse complications such as long waiting times, increased doses of immunosuppressive therapy, increased risk of infections and malignancies, high rates of acute rejection, and delayed graft function. Kidney graft failure is also associated with increasing the average waiting time for transplantation, due to relisting (15).
As of December 31, 2019, at the time ESOT was discussing this issue, ∼55,000 patients were on the transplantation waiting list in Europe (16), the vast majority of whom required kidney transplantation. Although ∼16% of transplantations performed in 21 European countries were re-transplants (9), data from Eurotransplant (which includes a different spread of countries) show that >20% of patients on the kidney waiting list required re-transplantation after failure of a prior graft (17). Longer waiting time on dialysis is an independent risk factor for death (18), and a considerable proportion of patients with graft failure die while waiting for re-transplantation. For example, in 2019, ∼10% of persons on the active Eurotransplant kidney waiting list were removed because they died or became unfit for transplantation (19).
While increasing longevity of kidney grafts could decrease the need for re-transplantation, importantly, the >20% of patients waitlisted for re-transplantation on Eurotransplant databases represents only those who are eligible for such procedures. Among European and US patients who experienced death-censored graft failure, 48% were waitlisted (median time 7.7 months) and 61% had HLA antibodies; most of the sensitized patients were not relisted for transplantation and remained on dialysis until death (20). A publication from Charité Hospital in Berlin found that between 1997 and 2017, 267 graft losses occurred in 254 patients, resulting in 117 (43.8%) relistings (21), of whom only 42 (35.9%) patients received a second transplant. At 5 years after graft loss, of the 254 patients, 49% had died, 27% were relisted, 14% were on dialysis and not relisted, and only 11% were re-transplanted (15).
Several studies demonstrate an increased mortality risk for patients who experience graft loss, compared with those with continued function (22–24) or those yet to receive a transplant (25). A study using competing-risk analysis confirmed a significantly increased all-cause mortality rate in patients relisted after graft failure compared with those awaiting a first transplant (16% vs. 11%; p = 0.033), with most deaths happening within 3 years of relisting (26). Prior transplant failure was associated with a 1.5-fold increased risk of mortality (95% confidence interval [CI] 1.01–2.2) (26).
However, a comparison of patients listed for first versus repeat transplantation does not account for the excess mortality rate seen in those who remain on lifelong dialysis after graft failure. Given that patients listed for re-transplantation are a selected population deemed capable of receiving another graft, it seems likely that those who are not relisted (primarily because of comorbidity and unacceptable risk) will have worse outcomes on dialysis. In addition, none of these analyses considers the burdens of returning to dialysis after failed transplantation, such as the costs associated with treatment (27), decreased ability to work and participate in society (28), and the psychological impact of returning to dialysis (29–31) (see also article by Tong et al. on patient reported outcome measures, in this Special Issue (32)).
Late Graft Failure: An Orphan Indication?
In addition, late graft failure could be considered as an orphan indication, when its occurrence is calculated in absolute terms with the general population as reference. A hypothetical steady-state situation, where the same number of grafts are failing as are being transplanted, would result in ∼21,000 graft losses per 512 million inhabitants in the EU, equivalent to four graft losses per 100,000 people, per year. This may fulfill the definition of an orphan indication and would do so even if twice as many graft losses were to occur.
Late Graft Failure: An Unmet Clinical Need
Death With a Functioning Graft
Death of the recipient with a functioning graft is the most important reason for graft loss, and is usually a primary safety endpoint in studies of interventions that aim to prolong kidney transplant function. The main causes of death with a functioning graft are cardiovascular disease (CVD) and over-immunosuppression resulting in adverse events such as malignancy or infection (33–35). The fact that over-immunosuppression can cause death is obvious. Importantly, the relatively common side effects of immunosuppressants (e.g., diabetes mellitus, hypertension, altered lipid profile, and nephrotoxicity leading to low glomerular filtration rate) can also increase CVD risk (35). Graft function can also directly impact CVD risk and mortality, which provides further evidence for the pivotal role of good kidney function in both graft and patient survival (36, 37). The negative impact of poor kidney function on mortality (and CVD mortality in particular) is also seen in the general population (38, 39).
Return to Dialysis/Re-Transplantation
Relative contributions of different pathological processes to graft failure have been evaluated (10, 33, 34, 40–42). Progression of fibrosis and accumulation of extracellular matrix i.e., interstitial fibrosis and tubular atrophy, IFTA) are key causes of graft loss. Fibrosis is thought to be mainly the consequence of nephron loss, and as aging is inevitably associated with a declining number of functioning nephrons, the quantity of nephrons might already be greatly reduced in grafts from marginal donors. After transplantation, nephrons can also be injured by immunological processes and/or other mechanisms (Figure 1) (43).
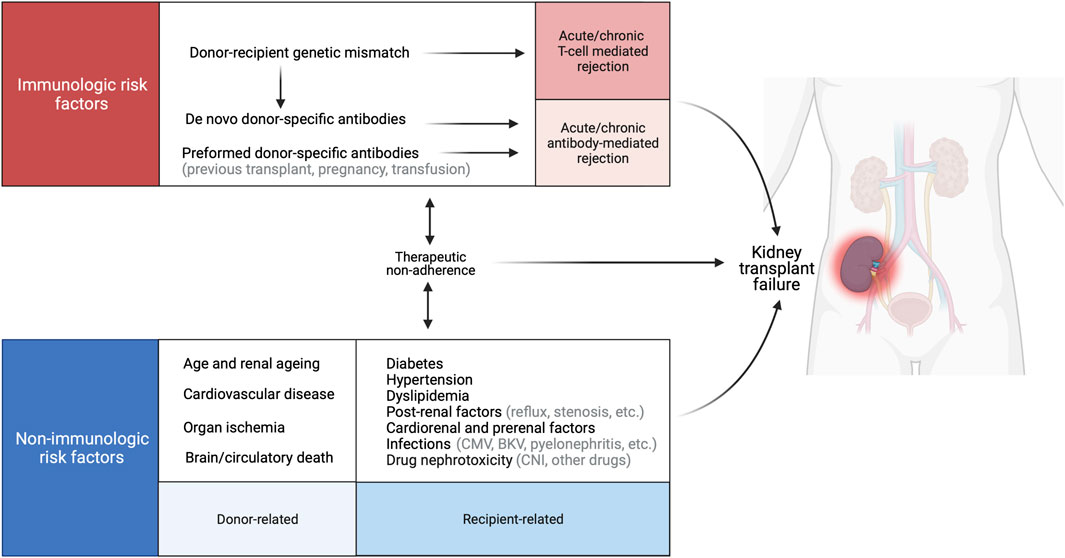
FIGURE 1. Causes of late allograft loss. Late graft failure is a multifactorial process that involves immunological factors related to the donor–recipient genetic mismatch, and nonimmunological factors that contribute to acute and chronic lesion development. BKV, BK virus; CMV, cytomegalovirus, CNI, calcineurin inhibitor. Created with BioRender.com.
Increasing evidence suggests a continuous alloimmune response to the donor graft, despite modern immunosuppression, unrelated to the patient’s level of adherence to immunotherapy. The incidence of acute cellular (i.e., T cell-mediated [TCMR]) rejection in the early months after transplantation is ∼10% and rarely leads to immediate graft loss if treated appropriately, but TCMR is also an important, relevant, risk factor for long-term graft loss (10). Chronic TCMR has been described as a pathological entity and seems associated with impaired outcome, but its true prevalence and importance remain poorly defined (4, 44). By contrast, AMR diagnosis—and individual parameters of AMR—clearly show detrimental long-term effects on the graft (3, 10). B cells play key roles in AMR as antibody-producing cells and antigen-presenting cells for T cells with indirect allospecificity (12, 45). Poor adherence to medication is a major contributor to AMR development (10), highlighting that behavioral and social factors have important immunological consequences (43, 46). Poor adherence to complex medication regimens is common: it is estimated that up to 25% of patients have some degree of nonadherence, with severe nonadherence recognized as being a major contributor to late graft failure (10, 47). Poor adherence is associated with donor-specific antibody (DSA) development and poor control of metabolic factors (46).
As histologic studies show that progressive fibrosis is a major cause of late graft loss, and because calcineurin inhibitors (CNIs) are known to cause fibrosis, it was proposed that late graft loss might be partly attributable to CNI nephrotoxicity (10, 48), causing nephron injury and ultimately nephron loss with striped fibrosis. Studies have tested the hypothesis that minimizing the CNI dose, or avoiding these agents altogether, might improve long-term graft survival rates. Although some research suggested that avoiding CNIs did not cause safety issues and was associated with improvement in renal function over time, others indicated increased acute TCMR and DSA development in patients on CNI-sparing or CNI-free regimens and minimal, if any, improvement in renal function (49, 50). Thus, our understanding of the relative contribution of CNIs as the main cause of late kidney graft loss has evolved, and we recognize that competing risks (e.g., increased rate of rejection, or DSA development) might limit the success of CNI-sparing regimens.
After alloimmune-mediated injury, recurrence of native kidney disease in the transplanted organ is another common cause of graft loss (10, 51). Some native kidney diseases (e.g., focal segmental glomerulosclerosis or diseases associated with inherited complement defects) recur frequently, often early after transplantation and with poor ensuing graft survival. Although all kidney diseases are capable of recurrence, most do not strongly affect graft survival in the early years following transplantation. Of note, an elevated risk of late graft loss was observed in patients with recurring glomerulonephritis (12).
Nonimmunologic factors that contribute to post-transplantation nephron damage include brain death of the donor, poor donor management, and cold and warm ischemia times (52–54); delayed graft function (55); and infections (e.g., polyomavirus [BKV], cytomegalovirus, pyelonephritis) (10, 34). Kidney transplant recipients also usually have a high burden of comorbidities, some caused by chronic uremia before and during dialysis. Contributions of some modifiable CVD risk factors to the progression of native kidney disease have been demonstrated unequivocally, but their effect on graft survival remains unclear because interventional studies are scarce. In competing-risk analyses, smoking, systolic blood pressure, and hemoglobin concentration remain as independent predictors of graft failure or doubling of creatinine level (12). Standard immunosuppressive regimens increase the risk of diabetes and hyperlipidemia, which appear to accelerate graft rejection independently of the potential effects of lipids on the graft vasculature (12).
Other factors that contribute to graft failure are reflux nephropathy or obstruction due to ureteral stenosis (10). Finally, poor graft quality (e.g., graft having lower reserves because of older donor age or expanded criteria donors) with lower nephron mass transplanted is an important baseline risk factor for late graft failure, as described previously (10).
Clearly, late graft failure is often a multifactorial process: active/acute diseases are additive and coincide with cumulative chronic injury (10, 12, 34, 56, 57). This chronic injury can also have many causes, increasing the vulnerability of grafts to superimposed acute injury. Acute and chronic factors (as described above) can injure the nephron; once this basic functional unit of the kidney is irreversibly damaged, it cannot be replaced, and renal function deteriorates. Hyperfiltration and glomerular hypertension of the remaining nephrons can lead to a vicious circle, with further reduction in functioning nephrons, as seen in native kidney disease. Although late graft failure is a heterogeneous condition, the underlying disease processes often share a common clinical pathway of declining kidney graft function (indicated by a declining glomerular filtration rate) and/or increasing proteinuria, with a rise in chronic histological injury and fibrosis.
Several studies highlight the importance of progressive fibrosis as a key pathway to graft failure and a target for intervention, independent of the recognized role of late AMR in graft failure (42, 44). Biopsies late after transplantation are particularly dominated by nonspecific chronic lesions and IFTA without displaying concomitant inflammation (44). Beyond 5–10 years after transplantation, failures become increasingly biased toward IFTA, which therefore represents a key finding among identifying factors involved in late graft failure. It is precisely these late failures that have proven so resistant to advances in transplantation practice (7, 9). However, underlying causes of IFTA and progressive nephron loss remain poorly understood: the histopathologic picture is complicated by issues including rejection phenomena and chronic CNI nephrotoxicity, together with under-investigated but clearly detrimental factors such as aging, viral infections, reflux, and pyelonephritis.
Progressive IFTA in the absence of inflammatory disease is a process once known as “mysterious dysregulated fibrosis” (40, 58). New insights have illuminated this process, which can involve epigenetic mechanisms, resulting in constitutive fibroblast activation (59), drug nephrotoxicity (60, 61) and other pathophysiological aspects (e.g., oxidative stress or innate immune activation (62)). Therapies directed toward progressive IFTA, which are emerging in the management of native kidney disease, should have some value after transplantation (62).
Unmet Needs: Interventions to Improve Late Graft Failure
Current immunosuppressive agents were approved for marketing based on studies with follow-up periods of <1 year. The approval of drugs that improved these short-term outcomes was based on research focusing on TCMR inhibition, which led to an important decline in early graft failure rates (7, 9) but did not substantially benefit long-term outcomes.
The impact of older immunosuppressive agents (e.g., cyclosporine) is not limited to short-term endpoints, however. Studies with ≥5-years follow-up periods, including cyclosporine withdrawal regimens, have demonstrated the effect of immunosuppressive drugs on long-term graft outcomes (63, 64). This suggests that different competing risks exist at different time points following transplantation. In addition, studies with tacrolimus have illustrated improved long-term outcomes compared with cyclosporine (65).
Very few randomized controlled trials (RCTs) have evaluated newer immunosuppressive agents (e.g., mTOR inhibitors, interleukin-2 receptor blockade, belatacept) with long-term graft survival as an endpoint. Extensions of the BENEFIT studies, reported at 7 and 10 years post transplantation (66, 67), demonstrated significantly lower risk of death or graft failure in the belatacept-treated group versus the cyclosporine-treated group, but only in standard criteria donor transplantations (67). Belatacept-treated patients had better outcomes despite having experienced more severe rejections (mainly TCMR) in the first year (66, 67), similar to findings of a study of early CNI withdrawal that included extensive follow-up (68). These studies clearly demonstrate the dissociation between TCMR and long-term outcome, suggesting that competing risks (e.g., cyclosporine toxicity, differences in metabolic profile, de novo DSA development) are more important than TCMR for long-term transplantation success.
Other studies had extended follow-up (beyond 1 year) after transplantation, comparing regimens of immunosuppressive agents that were approved based on short-term data. Although graft function sometimes improved over time, this did not reduce the rates of long-term graft failure (68, 69). Sometimes, worsening graft function and long-term graft survival rates were observed for the innovative regimen (70), which supports the hypothesis that long-term graft survival is affected by different competing risks at different time points. The complex reasons for graft loss (10), and the paucity of RCTs investigating the translation of short-term results into long-term survival benefits, highlight the difficulties in powering such trials sufficiently. Interpretation of long-term follow-up data is also confounded by frequent conversions to new, different immunosuppressive regimens.
Surrogate Endpoints for CMA Applications for Late Graft Failure
If CMA applications for novel drugs aiming at preventing or treating late graft failure are admissible to the EMA, the next discussion relates to the choice of the endpoints to be used for the required clinical trials. Graft failure is a highly relevant hard endpoint in clinical studies, but it is a late endpoint. This hampers the feasibility of using graft failure as an endpoint in clinical trials that aim at improving late graft failure rates.
Surrogates for late graft failure are therefore needed but require robust definitions. A good surrogate endpoint should fulfil four criteria: 1) The disease process is sufficiently understood; 2) The surrogate endpoint has biologic plausibility; 3) The strength of the consistency supports the relationship between the surrogate marker and outcome; 4) Treatment effects on the surrogate endpoint predict treatment effects on the clinical outcome of interest.
Kidney graft function and combined functional markers, donor-specific HLA antibodies and composite scores could be considered as surrogate endpoints, but do not fulfill all these criteria. For a detailed discussion on the potential acceptability of these surrogate endpoints for late graft failure, we refer to another manuscript in this Special Issue (6).
From Conditional to Full Marketing Authorization
After successful application for CMA of a product aimed at improving long-term graft survival, conversion to full marketing authorization is necessary, based on a post-marketing confirmatory commitment.
ESOT sees different options for this conversion of CMA to full marketing authorization. For example, applicants could consider requests for full marketing authorization based on long-term registration studies with accepted primary endpoints relating to graft rejection (2–4) function (5) and/or graft failure. Applicants could also consider requesting full marketing authorization based on comprehensive high-quality evidence from open-label study data, comparing findings to appropriate historic controls.
Alternatively, applicants could base the comprehensive evidence for full marketing authorization requests on good-quality data from registration studies, utilizing real-world data. Indeed, the EMA has already considered data from two other registries suitable for their decision-making processes: the European Cystic Fibrosis Society patient registry and the Cellular Therapy module of the European Blood and Marrow Transplant registry. The EMA Patient Registries Initiative (71) offers guidance on this topic. Of note, ESOT emphasizes that currently no European registries in kidney transplantation could be used as basis for requesting full marketing authorization.
A final option could be to use data from a qualified surrogate endpoint as a source of comprehensive evidence for a full marketing authorization request. Although CHMP/EMA has suggested to initiate a formal Qualification of Novel Methodologies procedure for e.g. the finalized iBox model (69) as a surrogate marker, this qualification is not yet achieved. The status and path toward formal qualification of composite scores as potential surrogate endpoints is discussed separately in this Special Issue (6).
Each of the above options for post-marketing commitments seems unsatisfactory at present, in the field of kidney transplantation. This may hamper the current admissibility of CMA applications for therapies aiming at reducing the incidence and burden of late kidney transplant failure. The results of formal qualification procedures are eagerly awaited and will hopefully change the landscape in future.
Conclusion
• Late graft failure (loss of graft function >1 year post transplant) is a condition with unmet medical need. Therefore, CMA should be considered for interventions that demonstrate potential benefits:
○ Late graft failure is a seriously debilitating, life-threatening disease for which no specific preventive or treatment options are available.
○ CMA of therapies aimed at preventing late graft failure could be based on trials that show benefit on a validated surrogate endpoint for graft failure.
• For drugs aimed at reducing late graft failure, applying for CMA could be considered.
○ CMA procedures facilitate timely access to new therapies.
○ Confirmatory post-marketing commitments will be needed to convert CMA to full marketing authorization.
Scientific Advice From the Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency (EMA) Regarding These Conclusions
• The CHMP agreed that improving long-term outcome after kidney transplantation is an area of unmet medical need; arguments for orphan designation of late graft failure were not followed.
• Should a novel therapy be proposed for CMA, the product will need to fulfil all of the following four criteria at the time CMA is considered: 1) positive benefit/risk balance; 2) it is likely that the applicant will be able to provide comprehensive data later; 3) unmet medical need is fulfilled; and 4) the benefit to public health of the medicinal product’s immediate availability on the market outweighs the risk due to need for further data.
• Criteria for CMA will be reviewed for specific data submitted; CMA cannot be granted a priori for any given product or indication.
Author Contributions
This article is one of several developed from the Broad Scientific Advice request, submitted to the EMA/CHMP by ESOT in 2020. For the present article, the working group on surrogate endpoints in kidney transplantation developed the ESOT position on the core question "Does CHMP agree that long-term outcome after kidney transplantation is an area of unmet medical need, for which conditional marketing authorization procedures should be considered, to facilitate timely access to new therapies? If so, does CHMP agree with the proposed surrogate endpoints for clinical trials for therapies requiring conditional marketing authorization?" The Centre for Evidence in Transplantation provided support with specific data extraction requests: these literature searches formed the basis of evidence used in the advice request and the present article. Input into the working group's output was provided from all ESOT members involved in the advice request process.
The present article was adapted by MN from the final Broad Scientific Advice request submission (June 2020), documentation from the meeting between ESOT and the CHMP Scientific Advice Working Party (SAWP) (September 2020), and the final response from the SAWP (December 2020). Drafts of the article were circulated to all co-authors for review and approval before submission.
Funding
This initiative was supported by the European Society for Organ Transplantation.
Conflict of Interest
LH reports speaker fees from Astellas, consultancy and research support from Chiesi, consultancy for Novartis, and research support from Sandoz. RO has received grants/research support from Amgen, Astellas, and Chiesi; and speakers' bureaux/honoraria from Amgen, Astellas, Chiesi, Hansa, Neovii, Novartis, and Teva. SS has received grants/research support from Bridge to Life, Chiesi, Neovii, Novartis, Organ Recovery Systems, and Sandoz; speakers' bureaux/honoraria from Astellas, BMS, Chiesi, Novartis, OrganOx, and Sanofi; and consulting fees from Astellas, Atara, Merck, NefroHealth, Novartis, Sandoz, and Teva. DG reports consultancy agreements and scientific boards for AstraZeneca, BMS, Hansa, and Sanofi. UH has received grants/research support from Baxter, Chiesi, and Neovii; speakers' bureaux/honoraria from Chiesi and Hansa; and consulting fees from Astellas, Hansa, Neovii, Novartis, and Teva. IJ's institution has received speaker's fees from XVIVO Perfusion. MR has received lecture fees from Astellas and Chiesi; and research grant support (paid to institution) from Astellas and Chiesi for investigator-initiated studies. SS has received grants/research support from Bridge to Life, Chiesi, Neovii, Novartis, Organ Recovery Systems, and Sandoz; speakers' bureaux/honoraria from Astellas, BMS, Chiesi, Novartis, OrganOx, and Sanofi; and consulting fees from Astellas, Atara, Merck, NefroHealth, Novartis, Sandoz, and Teva. KB has received honoraria and/or research funding from Alexion, Astellas, Bristol Myers Squibb, Chiesi, Fresenius, Hansa, Hexal, Merck, Novartis, Otsuka, Pfizer, Roche, Sandoz, Siemens, and Veloxis.
The remaining authors declare that the work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank the experts involved with the European Medicines Agency (EMA) Committee for Medicinal Products for Human Use (CHMP) who participated in the Broad Scientific Advice request. The published information is based on EMA feedback received during the Broad Scientific Advice request. EMA/CHMP have not been involved in the drafting or review of the manuscript to be published. This publication does not constitute a formal EMA/CHMP endorsement of the manuscript. Medical writing support was provided by Linda Edmondson, independent medical writer, funded by ESOT.
References
1.European Medicines Agency. Clinical Investigation of Immunosuppressants for Solid Organ Transplantation (2008). CHMP/EWP/263148/06. Available at: https://www.ema.europa.eu/en/clinical-investigation-immunosuppressants-solid-organ-transplantation (Accessed February 8, 2022).
2. Becker, JU, Seron, D, Rabant, M, Roufosse, C, and Naesens, M. Evolution of the Definition of Rejection in Kidney Transplantation and Its Use as an Endpoint in Clinical Trials. Transpl Int (2022) 35. doi:10.3389/ti.2022.10141
3. Roufosse, C, Becker, JU, Rabant, M, Seron, D, Bellini, MI, Böhmig, G, et al. Proposed Definitions of Antibody-Mediated Rejection for Use as a Clinical Trial Endpoint in Kidney Transplantation. Transpl Int (2022) 35. doi:10.3389/ti.2022.10140
4. Seron, D, Rabant, M, Becker, JU, Roufosse, C, Bellini, MI, Böhmig, G, et al. Proposed Definitions of T Cell-Mediated Rejection and Tubulointerstitial Inflammation as Clinical Trial Endpoints in Kidney Transplantation. Transpl Int (2022) 35. doi:10.3389/ti.2022.10135
5. Hilbrands, L, Budde, K, Bellini, MI, Diekmann, F, Furian, L, Grinyó, J, et al. Allograft Function as Endpoint for Clinical Trials in Kidney Transplantation. Transpl Int (2022) 35. doi:10.3389/ti.2022.10139
6. Naesens, M, Budde, K, Hilbrands, L, Oberbauer, R, Bellini, MI, Glotz, D, et al. Surrogate Endpoints for Late Kidney Transplantation Failure. Transpl Int (2022) 35. doi:10.3389/ti.2022.10136
7. Lamb, KE, Lodhi, S, and Meier-Kriesche, H-U. Long-term Renal Allograft Survival in the United States: a Critical Reappraisal. Am J Transpl (2011) 11:450–62. doi:10.1111/j.1600-6143.2010.03283.x
8. Naesens, M, and Thaunat, O. BENEFIT of Belatacept: Kidney Transplantation Moves Forward. Nat Rev Nephrol (2016) 12:261–2. doi:10.1038/nrneph.2016.34
9. Coemans, M, Süsal, C, Döhler, B, Anglicheau, D, Giral, M, Bestard, O, et al. Analyses of the Short- and Long-Term Graft Survival after Kidney Transplantation in Europe between 1986 and 2015. Kidney Int (2018) 94:964–73. doi:10.1016/j.kint.2018.05.018
10. Mayrdorfer, M, Liefeldt, L, Wu, K, Rudolph, B, Zhang, Q, Friedersdorff, F, et al. Exploring the Complexity of Death-Censored Kidney Allograft Failure. J Am Soc Nephrol (2021) 32:1513–26. doi:10.1681/asn.2020081215
11.European Medicines Agency. Conditional Marketing Authorization (2022). Available at: https://www.ema.europa.eu/en/human-regulatory/marketing-authorisation/conditional-marketing-authorisation (Accessed February 8, 2022).
12. Wekerle, T, Segev, D, Lechler, R, and Oberbauer, R. Strategies for Long-Term Preservation of Kidney Graft Function. The Lancet (2017) 389:2152–62. doi:10.1016/s0140-6736(17)31283-7
13.Agence de la Biomedicine. Annual Report (2017). Available at: https://www.agence-biomedecine.fr/annexes/bilan2017/donnees/organes/06-rein/synthese.htm (Accessed February 8, 2022).
14. Süsal, C, Döhler, B, and Opelz, G. Presensitized Kidney Graft Recipients with HLA Class I and II Antibodies Are at Increased Risk for Graft Failure: a Collaborative Transplant Study Report. Hum Immunol (2009) 70:569–73. doi:10.1016/j.humimm.2009.04.013
15. Schrezenmeier, E, Lehner, LJ, Merkel, M, Mayrdorfer, M, Duettmann, W, Naik, MG, et al. What Happens after Graft Loss? A Large, Long‐term, Single‐center Observation. Transpl Int (2021) 34:732–42. doi:10.1111/tri.13834
16.DG SANTE, European Commission. Organs, Blood, Tissues & Cells in the EU (2022). Available at: https://ec.europa.eu/health//sites/health/files/blood_tissues_organs/docs/infographic_obtc_en.pdf (Accessed February 8, 2022).
17.Eurotransplant statistics library (2021). Available at: https://www.eurotransplant.org/statistics/statistics-library/ (Accessed February 8, 2022).
18. Haller, MC, Kainz, A, Baer, H, and Oberbauer, R. Dialysis Vintage and Outcomes after Kidney Transplantation: a Retrospective Cohort Study. Clin J Am Soc Nephrol (2017) 12:122–30. doi:10.2215/cjn.04120416
19.Eurotransplant. (2019). Available at: https://www.eurotransplant.org/annual-report/annual-report-2019/ (Accessed February 8, 2022). Annual Report.
20. Rose, C, Schaeffner, E, Frei, U, Gill, J, and Gill, JS. A Lifetime of Allograft Function with Kidneys from Older Donors. J Am Soc Nephrol (2015) 26:2483–93. doi:10.1681/asn.2014080771
21. Halleck, F, Merkel, M, Bach, P, Niemann, M, Lachmann, N, Lehner, L, et al. Epitope Matching Predicts Immunization after Allograft Failure Causing Longer Waiting Time for Re-transplantation. ERA-EDTA 2019 Congress Abstracts Library; SaO017 (2022). Available at: https://atcmeetingabstracts.com/abstract/epitop-matching-predicts-immunization-in-kidney-transplant-recipients-with-allograft-failure-leading-to-worse-outcomes/ (Accessed February 8, 2022).
22. Kaplan, B, and Meier-Kriesche, H-U. Death after Graft Loss: an Important Late Study Endpoint in Kidney Transplantation. Am J Transpl (2002) 2:970–4. doi:10.1034/j.1600-6143.2002.21015.x
23. Rao, PS, Schaubel, DE, and Saran, R. Impact of Graft Failure on Patient Survival on Dialysis: a Comparison of Transplant-Naive and post-graft Failure Mortality Rates. Nephrol Dial Transplant (2005) 20:387–91. doi:10.1093/ndt/gfh595
24. Rao, PS, Schaubel, DE, Jia, X, Li, S, Port, FK, and Saran, R. Survival on Dialysis post-kidney Transplant Failure: Results from the Scientific Registry of Transplant Recipients. Am J Kidney Dis (2007) 49:294–300. doi:10.1053/j.ajkd.2006.11.022
25. Perl, J, Zhang, J, Gillespie, B, Wikstrom, B, Fort, J, Hasegawa, T, et al. Reduced Survival and Quality of Life Following Return to Dialysis after Transplant Failure: the Dialysis Outcomes and Practice Patterns Study. Nephrol Dial Transplant (2012) 27:4464–72. doi:10.1093/ndt/gfs386
26. Hernández, D, Muriel, A, Castro de la Nuez, P, Alonso-titos, J, Ruiz-Esteban, P, Duarte, A, et al. Survival in Southern European Patients Waitlisted for Kidney Transplant after Graft Failure: a Competing Risk Analysis. PLoS One (2018) 13:e0193091. doi:10.1371/journal.pone.0193091
27. Vanholder, R, Davenport, A, Hannedouche, T, Kooman, J, Kribben, A, Lameire, N, et al. Reimbursement of Dialysis: a Comparison of Seven Countries. J Am Soc Nephrol (2012) 23:1291–8. doi:10.1681/asn.2011111094
28. Erickson, KF, Zhao, B, Ho, V, and Winkelmayer, WC. Employment Among Patients Starting Dialysis in the United States. Clin J Am Soc Nephrol (2018) 13:265–73. doi:10.2215/cjn.06470617
29. Palmer, S, Vecchio, M, Craig, JC, Tonelli, M, Johnson, DW, Nicolucci, A, et al. Prevalence of Depression in Chronic Kidney Disease: Systematic Review and Meta-Analysis of Observational Studies. Kidney Int (2013) 84:179–91. doi:10.1038/ki.2013.77
30. Tong, A, Hanson, CS, Chapman, JR, Halleck, F, Budde, K, Josephson, MA, et al. 'Suspended in a Paradox'-Patient Attitudes to Wait-Listing for Kidney Transplantation: Systematic Review and Thematic Synthesis of Qualitative Studies. Transpl Int (2015) 28:771–87. doi:10.1111/tri.12575
31. Tong, A, Gill, J, Budde, K, Marson, L, Reese, PP, Rosenbloom, D, et al. Toward Establishing Core Outcome Domains for Trials in Kidney Transplantation. Transplantation (2017) 101:1887–96. doi:10.1097/tp.0000000000001774
32. Tong, A, Oberbauer, R, Bellini, MI, Budde, K, Caskey, FJ, Dobbels, F, et al. Patient-Reported Outcomes as Endpoints in Clinical Trials of Kidney Transplantation Interventions. Transpl Int (2022) 35. doi:10.3389/ti.2022.10134
33. El-Zoghby, ZM, Stegall, MD, Lager, DJ, Kremers, WK, Amer, H, Gloor, JM, et al. Identifying Specific Causes of Kidney Allograft Loss. Am J Transpl (2009) 9:527–35. doi:10.1111/j.1600-6143.2008.02519.x
34. Van Loon, E, Senev, A, Lerut, E, Coemans, M, Callemeyn, J, Van Keer, JM, et al. Assessing the Complex Causes of Kidney Allograft Loss. Transplantation (2020) 104:2557–66. doi:10.1097/tp.0000000000003192
35. Liefeldt, L, and Budde, K. Risk Factors for Cardiovascular Disease in Renal Transplant Recipients and Strategies to Minimize Risk. Transpl Int (2010) 23:1191–204. doi:10.1111/j.1432-2277.2010.01159.x
36. Fellstrom, B, Jardine, AG, Soveri, I, Cole, E, Neumayer, H-H, Maes, B, et al. Renal Dysfunction Is a strong and Independent Risk Factor for Mortality and Cardiovascular Complications in Renal Transplantation. Am J Transpl (2005) 5:1986–91. doi:10.1111/j.1600-6143.2005.00983.x
37. Soveri, I, Snyder, J, Holdaas, H, Holme, I, Jardine, AG, L’Italien, GJ, et al. The External Validation of the Cardiovascular Risk Equation for Renal Transplant Recipients. Transplantation (2013) 95:142–7. doi:10.1097/tp.0b013e31827722c9
38. Badve, SV, Palmer, SC, Hawley, CM, Pascoe, EM, Strippoli, GFM, and Johnson, DW. Glomerular Filtration Rate Decline as a Surrogate End point in Kidney Disease Progression Trials. Nephrol Dial Transpl (2016) 31:1425–36. doi:10.1093/ndt/gfv269
39. Astor, BC, Matsushita, K, Matsushita, K, Gansevoort, RT, van der Velde, M, Woodward, M, et al. Lower Estimated Glomerular Filtration Rate and Higher Albuminuria Are Associated with Mortality and End-Stage Renal Disease. A Collaborative Meta-Analysis of Kidney Disease Population Cohorts. Kidney Int (2011) 79:1331–40. doi:10.1038/ki.2010.550
40. Sellarés, J, De Freitas, DG, Mengel, M, Reeve, J, Einecke, G, Sis, B, et al. Understanding the Causes of Kidney Transplant Failure: the Dominant Role of Antibody-Mediated Rejection and Nonadherence. Am J Transpl (2012) 12:388–99. doi:10.1111/j.1600-6143.2011.03840.x
41. Naesens, M, Kuypers, DRJ, De Vusser, K, Evenepoel, P, Claes, K, Bammens, B, et al. The Histology of Kidney Transplant Failure. Transplantation (2014) 98:427–35. doi:10.1097/tp.0000000000000183
42. Chand, S, Atkinson, D, Collins, C, Briggs, D, Ball, S, Sharif, A, et al. The Spectrum of Renal Allograft Failure. PLoS One (2016) 11:e0162278. doi:10.1371/journal.pone.0162278
43. Neuberger, JM, Bechstein, WO, Kuypers, DR, Burra, P, Citterio, F, De Geest, S, et al. Practical Recommendations for Long-Term Management of Modifiable Risks in Kidney and Liver Transplant Recipients: a Guidance Report and Clinical Checklist by the Consensus on Managing Modifiable Risk in Transplantation (COMMIT) Group. Transplantation (2017) 101(4S Suppl. 2):S1–56. doi:10.1097/TP.0000000000001651
44. Haas, M, Loupy, A, Lefaucheur, C, Roufosse, C, Glotz, D, Seron, D, et al. The Banff 2017 Kidney Meeting Report: Revised Diagnostic Criteria for Chronic Active T Cell-Mediated Rejection, Antibody‐mediated Rejection, and Prospects for Integrative Endpoints for Next‐generation Clinical Trials. Am J Transpl (2018) 18:293–307. doi:10.1111/ajt.14625
45. Loupy, A, and Lefaucheur, C. Antibody-mediated Rejection of Solid-Organ Allografts. N Engl J Med (2018) 379:1150–60. doi:10.1056/nejmra1802677
46. Gokoel, SRM, Gombert-Handoko, KB, Zwart, TC, van der Boog, PJM, Moes, DJAR, and de Fijter, JW. Medication Non-adherence after Kidney Transplantation: A Critical Appraisal and Systematic Review. Transplant Rev (2020) 34:100511. doi:10.1016/j.trre.2019.100511
47. Morath, C, Opelz, G, Zeier, M, and Süsal, C. Prevention of Antibody-Mediated Kidney Transplant Rejection. Transpl Int (2012) 25:633–45. doi:10.1111/j.1432-2277.2012.01490.x
48. Jevnikar, AM, and Mannon, RB. Late Kidney Allograft Loss: what We Know about it, and what We Can Do about it. Clin J Am Soc Nephrol (2008) 3(Suppl. 2):S56–67. doi:10.2215/CJN.03040707
49. Sharif, A, Shabir, S, Chand, S, Cockwell, P, Ball, S, and Borrows, R. Meta-analysis of Calcineurin-Inhibitor-Sparing Regimens in Kidney Transplantation. J Am Soc Nephrol (2011) 22:2107–18. doi:10.1681/asn.2010111160
50. Lim, WH, Eris, J, Kanellis, J, Pussell, B, Wiid, Z, Witcombe, D, et al. A Systematic Review of Conversion from Calcineurin Inhibitor to Mammalian Target of Rapamycin Inhibitors for Maintenance Immunosuppression in Kidney Transplant Recipients. Am J Transpl (2014) 14:2106–19. doi:10.1111/ajt.12795
51. Briganti, EM, Russ, GR, McNeil, JJ, Atkins, RC, and Chadban, SJ. Risk of Renal Allograft Loss from Recurrent Glomerulonephritis. N Engl J Med (2002) 347:103–9. doi:10.1056/nejmoa013036
52. Summers, DM, Johnson, RJ, Allen, J, Fuggle, SV, Collett, D, Watson, CJ, et al. Analysis of Factors that Affect Outcome after Transplantation of Kidneys Donated after Cardiac Death in the UK: a Cohort Study. The Lancet (2010) 376:1303–11. doi:10.1016/s0140-6736(10)60827-6
53. Heylen, L, Jochmans, I, Samuel, U, Tieken, I, Naesens, M, Pirenne, J, et al. The Duration of Asystolic Ischemia Determines the Risk of Graft Failure after Circulatory-Dead Donor Kidney Transplantation: a Eurotransplant Cohort Study. Am J Transpl (2018) 18:881–9. doi:10.1111/ajt.14526
54. Krishnan, AR, Wong, G, Chapman, JR, Coates, PT, Russ, GR, Pleass, H, et al. Prolonged Ischemic Time, Delayed Graft Function, and Graft and Patient Outcomes in Live Donor Kidney Transplant Recipients. Am J Transpl (2016) 16:2714–23. doi:10.1111/ajt.13817
55. Butala, NM, Reese, PP, Doshi, MD, and Parikh, CR. Is Delayed Graft Function Causally Associated with Long-Term Outcomes after Kidney Transplantation? Instrumental Variable Analysis. Transplantation (2013) 95:1008–14. doi:10.1097/tp.0b013e3182855544
56. Legendre, C, Canaud, G, and Martinez, F. Factors Influencing Long-Term Outcome after Kidney Transplantation. Transpl Int (2014) 27:19–27. doi:10.1111/tri.12217
57. Van Loon, E, Lerut, E, and Naesens, M. The Time Dependency of Renal Allograft Histology. Transpl Int (2017) 30:1081–91. doi:10.1111/tri.13042
58. Naesens, M, and Lerut, E. Looking Back to Evaluate the Causes of Graft Loss? A Response to Dr. Halloran and Dr. Sellares.Am J Transpl (2013) 13:1933–4. doi:10.1111/ajt.12316
59. Bechtel, W, McGoohan, S, Zeisberg, EM, Müller, GA, Kalbacher, H, Salant, DJ, et al. Methylation Determines Fibroblast Activation and Fibrogenesis in the Kidney. Nat Med (2010) 16:544–50. doi:10.1038/nm.2135
60. Chapman, JR. Chronic Calcineurin Inhibitor Nephrotoxicity-Lest We Forget. Am J Transpl (2011) 11:693–7. doi:10.1111/j.1600-6143.2011.03504.x
61. Naesens, M, Kuypers, DRJ, and Sarwal, M. Calcineurin Inhibitor Nephrotoxicity. Clin J Am Soc Nephrol (2009) 4:481–508. doi:10.2215/cjn.04800908
62. Boor, P, and Floege, J. Renal Allograft Fibrosis: Biology and Therapeutic Targets. Am J Transpl (2015) 15:863–86. doi:10.1111/ajt.13180
63. Gallagher, M, Jardine, M, Perkovic, V, Cass, A, McDonald, S, Petrie, J, et al. Cyclosporine Withdrawal Improves Long-Term Graft Survival in Renal Transplantation. Transplantation (2009) 87:1877–83. doi:10.1097/tp.0b013e3181a76823
64. Kreis, H, Oberbauer, R, Campistol, JM, Mathew, T, Daloze, P, Schena, FP, et al. Long-term Benefits with Sirolimus-Based Therapy after Early Cyclosporine Withdrawal. J Am Soc Nephrol (2004) 15:809–17. doi:10.1097/01.asn.0000113248.59077.76
65. Jurewicz, WA. Tacrolimus versus Cyclosporin Immunosuppression: Long-Term Outcome in Renal Transplantation. Nephrol Dial Transpl (2003) 18(Suppl. 1):i7–11. doi:10.1093/ndt/gfg1028
66. Vincenti, F, Blancho, G, Durrbach, A, Grannas, G, Grinyó, J, Meier-Kriesche, H-U, et al. Ten-year Outcomes in a Randomized Phase II Study of Kidney Transplant Recipients Administered Belatacept 4-weekly or 8-weekly. Am J Transpl (2017) 17:3219–27. doi:10.1111/ajt.14452
67. Durrbach, A, Pestana, JM, Florman, S, Del Carmen Rial, M, Rostaing, L, Kuypers, D, et al. Long-term Outcomes in Belatacept- versus Cyclosporine-Treated Recipients of Extended Criteria Donor Kidneys: Final Results from BENEFIT-EXT, a Phase Iii Randomized Study. Am J Transpl (2016) 16:3192–201. doi:10.1111/ajt.13830
68. Budde, K, Lehner, F, Sommerer, C, Reinke, P, Arns, W, Eisenberger, U, et al. Five-year Outcomes in Kidney Transplant Patients Converted from Cyclosporine to Everolimus: the Randomized ZEUS Study. Am J Transpl (2014) 15:119–28. doi:10.1111/ajt.12952
69. Sommerer, C, Duerr, M, Witzke, O, Lehner, F, Arns, W, Kliem, V, et al. Five-year Outcomes in Kidney Transplant Patients Randomized to Everolimus with Cyclosporine Withdrawal or Low-Exposure Cyclosporine versus Standard Therapy. Am J Transpl (2018) 18:2965–76. doi:10.1111/ajt.14897
70. Chhabra, D, Skaro, AI, Leventhal, JR, Dalal, P, Shah, G, Wang, E, et al. Long-term Kidney Allograft Function and Survival in Prednisone-free Regimens: Tacrolimus/mycophenolate Mofetil versus Tacrolimus/sirolimus. Clin J Am Soc Nephrol (2012) 7:504–12. doi:10.2215/cjn.06940711
71.EMA Human Regulatory: Patient Registries (2021). Available at: https://www.ema.europa.eu/en/human-regulatory/post-authorisation/patient-registries (Accessed February 8, 2022).
Keywords: mortality, late graft failure, unmet medical need, morbidity, re-transplantation, clinical studies
Citation: Naesens M, Loupy A, Hilbrands L, Oberbauer R, Bellini MI, Glotz D, Grinyó J, Heemann U, Jochmans I, Pengel L, Reinders M, Schneeberger S and Budde K (2022) Rationale for Surrogate Endpoints and Conditional Marketing Authorization of New Therapies for Kidney Transplantation. Transpl Int 35:10137. doi: 10.3389/ti.2022.10137
Received: 21 October 2021; Accepted: 10 March 2022;
Published: 20 May 2022.
Copyright © 2022 Naesens, Loupy, Hilbrands, Oberbauer, Bellini, Glotz, Grinyó, Heemann, Jochmans, Pengel, Reinders, Schneeberger and Budde. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maarten Naesens, bWFhcnRlbi5uYWVzZW5zQGt1bGV1dmVuLmJl